The NCCPA™ Gastroenterology and Nutrition PANCE Content Blueprint covers five topics under the category diseases of the small intestine
| Appendicitis (ReelDx) | ReelDx Virtual Rounds (Appendicitis )Patient will present as → a 14-year-old boy with nausea, vomiting, constipation, and periumbilical pain that has settled in the lower right quadrant. The patient’s mom gave him a piece of toast and some water about 5 hours ago but he vomited 30 minutes after eating. On physical exam, he has tenderness and guarding in the lower right quadrant, pain upon flexion and internal rotation of right lower extremity, RLQ pain with right hip extension, and RLQ pain with palpation of the LLQ. Blood tests reveal leukocytosis with a shift to the left. Appendicitis is the inflammation of the appendix, typically due to obstruction of the appendiceal lumen, leading to infection and possible perforation
Signs:
DX: Clinical diagnosis:
TX: surgical appendectomy  CT scan of the abdomen showing an enlarged appendix, suggestive of acute appendicitis. |
| Celiac disease and gluten intolerance | Patient will present as → a 34-year-old male presents to the clinic with a six-month history of chronic diarrhea, weight loss, and generalized weakness. He reports frequent abdominal pain and bloating after meals. He has also noticed a blistering, itchy rash on his elbows and knees. His medical history is significant for iron deficiency anemia. Physical examination reveals pallor, a distended abdomen, and a rash consistent with dermatitis herpetiformis. Laboratory tests show low hemoglobin and hematocrit levels, elevated transaminases, and a positive tissue transglutaminase (tTG) IgA antibody. Given his clinical presentation and positive serologic test for celiac disease, the patient is diagnosed with celiac disease. Upper endoscopy with a biopsy of the small intestine is scheduled to confirm villous atrophy. He is started on a strict gluten-free diet and referred to a dietitian for comprehensive dietary education and management. He is also advised to avoid foods that may contain hidden sources of gluten and to be aware of cross-contamination. Follow-up is planned to monitor his response to the gluten-free diet, check for improvement in symptoms, and reassess his nutritional status. Celiac Disease is an autoimmune disorder triggered by gluten ingestion, leading to inflammation and damage of the small intestine
DX:
TX: A strict lifelong gluten-free diet (avoiding wheat, barley, rye)
Non-Celiac Gluten Sensitivity (NCGS): A condition causing symptoms similar to celiac disease, such as bloating and abdominal pain, WITHOUT the autoimmune intestinal damage. Diagnosed by ruling out celiac disease and wheat allergy, and observing symptom improvement on a gluten-free diet. Gluten sensitivity levels vary, and some individuals may tolerate minimal gluten.
|
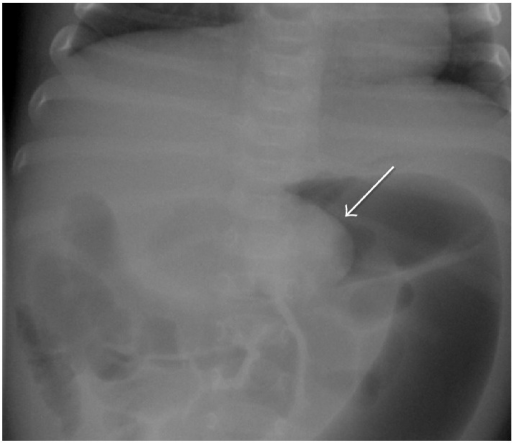
| Intussusception (ReelDx) | ReelDx Virtual Rounds (Intussusception)Patient will present as → a young mother who brings her 12-month-old daughter to your office, reporting that she has had recurrent “belly aches” for the past two weeks. The child experiences sudden, colicky abdominal pain that recurs every 15 to 20 minutes, often with vomiting. These episodes are interspersed with periods of no complaints. The mother also reports that she has seen her squatting with her knees to her chest, which seems to relieve her of her symptoms. She describes her stool as bloody with mucus, almost as though it were a currant jelly. On physical examination, you note abdominal distention and tenderness along with a sausage-shaped abdominal mass in the RUQ. Ultrasound shows a target sign, confirming intussusception. Management includes fluid resuscitation and air enema reduction, with surgical intervention if nonoperative reduction fails. Intussusception is the telescoping of one segment of the intestine into another, leading to bowel obstruction and compromised blood flow
DX: Diagnosis is made with abdominal ultrasound, showing the classic “target” or “donut” sign TX: Air or contrast enema is both diagnostic and therapeutic in most pediatric cases
|
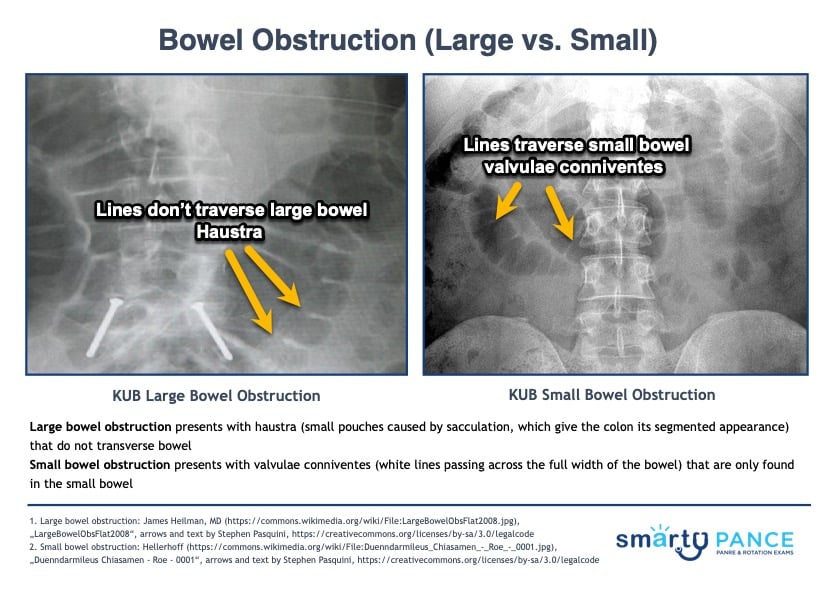
| Small bowel obstruction | ReelDx Virtual Rounds (Small bowel obstruction)Patient with small bowel obstruction will present as → a 55-year-old male presents to the emergency department with a two-day history of severe abdominal pain, vomiting, and inability to pass stool or gas. He describes the pain as crampy and worsening, localized initially around the umbilicus but now diffused across the abdomen. His medical history is significant for an open appendectomy 20 years ago. On examination, his abdomen is distended and tender with high-pitched, tinkling bowel sounds. He is afebrile, but his heart rate is elevated. An abdominal X-ray reveals dilated loops of small bowel with air-fluid levels. You note valvulae conniventes across the full width of the bowel suggestive of a small bowel obstruction. A CT scan of the abdomen confirms the diagnosis, showing a transition point with no evidence of strangulation. The patient is admitted for nasogastric decompression, intravenous fluids, and bowel rest. Surgery is consulted for potential operative intervention, given his history of previous abdominal surgery and the likelihood of adhesive disease. The patient is closely monitored for signs of bowel ischemia or perforation. 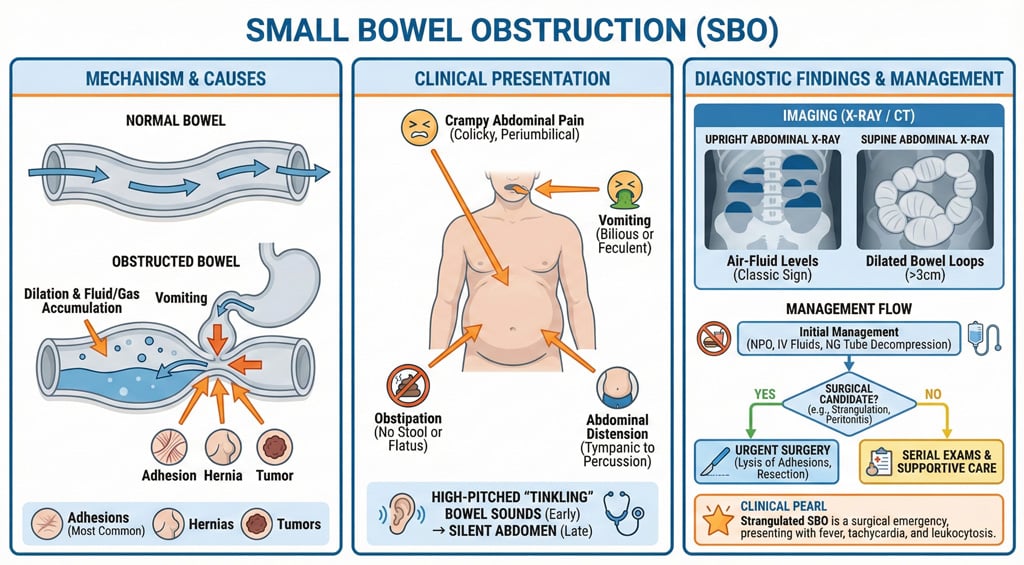 Small bowel obstruction Small bowel obstruction
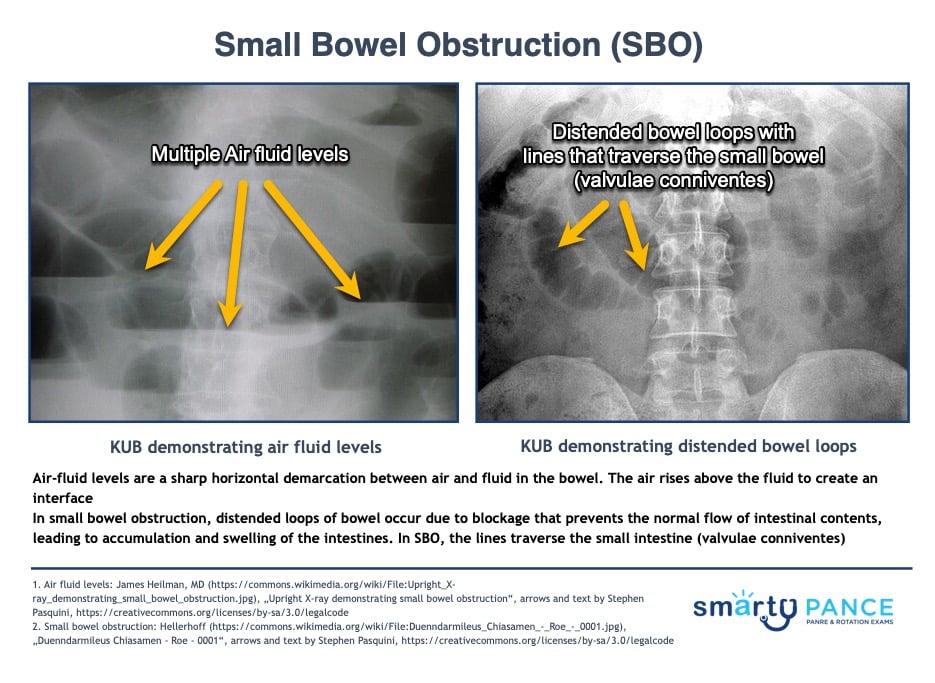
DX: Obtain plain radiographs to quickly confirm a diagnosis of bowel obstruction, and, provided the films do not have findings that indicate the need for immediate intervention, then use computed tomography (CT) of the abdomen and pelvis to further characterize the nature, severity, and potential etiologies of the obstruction
TX: Treat with decompression with an NGT, bowel rest, surgery if a mechanical obstruction is suspected Hyperactive bowel sounds, as heard in SBO SBO vs. LBO On the physical exam:
On the abdominal x-ray (KUB):
|
| Polyps of small bowel | Patient will present as → a 45-year-old woman presents with intermittent, crampy abdominal pain and iron-deficiency anemia. She experiences occasional nausea but no vomiting, weight loss, or bowel habit changes. Her medical history and physical examination, including a soft, non-distended abdomen, are unremarkable. Despite normal upper endoscopy and colonoscopy results, persistent symptoms and anemia lead to a capsule endoscopy, revealing a 2 cm jejunal polyp. A double-balloon enteroscopy confirms it as a benign hamartomatous polyp. She undergoes successful endoscopic polypectomy, resolving her symptoms and anemia, with planned follow-up for symptom monitoring. Small bowel polyps are abnormal growths of tissue protruding from the lining of the small intestine
DX: Small bowel polyps are often found incidentally during endoscopy, surgery, or imaging for other indications
TX: Most small hyperplastic polyps can just be followed without intervention
|



{kind=link}