The NCCPA™ Gastroenterology and Nutrition PANCE Content Blueprint covers acute and chronic pancreatitis under the category disorders of the pancreas
| Acute and chronic pancreatitis | Patient will present as → a 37-year-old male complaining of rapid onset of severe mid-epigastric pain with radiation to the back after eating a large meal. The pain typically lessens when the patient leans forward or lies in the fetal position. Physical exam shows low-grade fever, epigastric tenderness, diminished bowel sounds, and bruising of the flanks. An abdominal CT scan shows localized dilation of the upper duodenum and a small collection of fluid in the left pleural cavity.
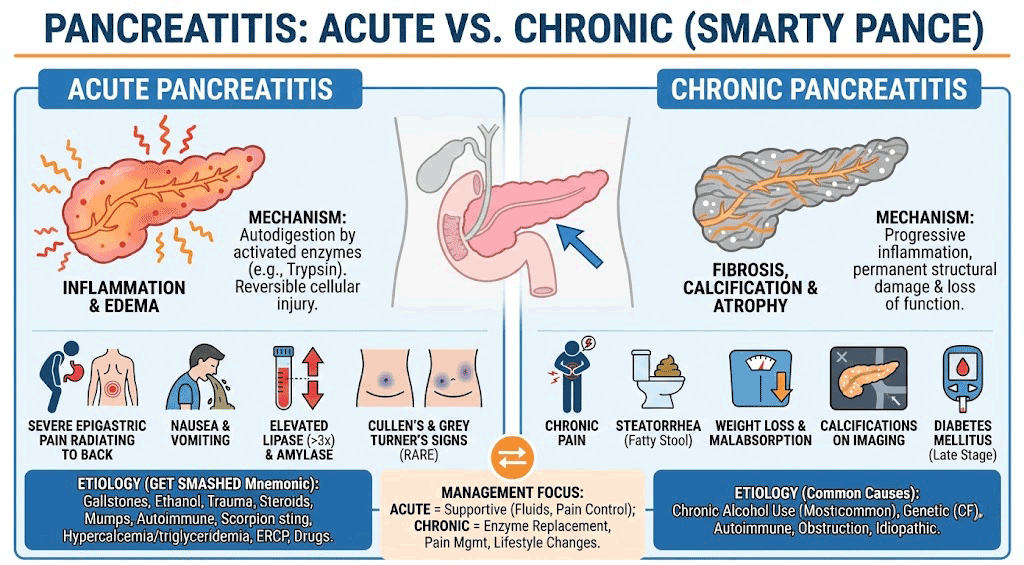
Acute pancreatitis is most commonly caused by gallstones (most common overall) and alcohol (most common in men), diagnosed by 2 of 3 criteria: epigastric pain radiating to the back + lipase ≥3× ULN + characteristic CT findings; Ranson's criteria and BISAP score predict severity; hemorrhagic pancreatitis produces Grey Turner's sign (flank ecchymosis) and Cullen's sign (periumbilical ecchymosis); treatment is aggressive IV fluids, pain control, NPO, and early enteral nutrition for severe cases.
DX: Diagnosis requires 2 of 3: (1) characteristic pain, (2) lipase ≥ 3× normal (most specific), (3) imaging findings; CT abdomen = best initial imaging if diagnosis unclear or severe
 This 40-year-old woman complained of worsening epigastric pain of five days duration. On examination, she had hypotension, a board-like abdomen, and extensive ecchymosis over her right loin (Grey Turner’s sign)  Acute pancreatitis with Cullen’s sign Severity assessment: use BISAP or Ranson criteria Ranson’s criteria for poor prognosis: At admit:
At 48 hrs:
TX: Aggressive IV fluids (lactated Ringer’s), NPO, and IV opioids for pain control; early fluids are the most important mortality-reducing step
Chronic Pancreatitis Patient will present as → a 45-year-old man with a long history of alcohol use presenting with chronic epigastric pain radiating to the back, worse after meals, along with weight loss and bulky, foul-smelling stools (steatorrhea). Over time he develops diabetes mellitus. CT scan shows pancreatic calcifications. He is treated with pancreatic enzyme replacement (pancrelipase), alcohol cessation, pain control, and fat-soluble vitamin supplementation. Chronic pancreatitis is progressive inflammatory fibrosis of the pancreas leading to irreversible exocrine and endocrine dysfunction (most commonly due to chronic alcohol use).
DX: CT scan = best initial test showing pancreatic calcifications; fecal elastase ↓ confirms exocrine insufficiency (functional test)
TX: Pancreatic enzyme replacement (pancrelipase) + alcohol and smoking cessation + pain control (stepwise, avoid opioids if possible)
PEARLS:
|
{kind=link}
{kind=link}