 Lecture
LecturePatient will present as → an elderly bed-bound patient with impaired mental function and poor fluid/fiber intake who complains of incontinence of liquid stool. He also reports rectal pressure and lower abdominal pain. The pain is cramping in quality and the patient’s abdomen is “bloated.” Digital rectal examination reveals a large amount of stool in the rectum.

To watch this and all of Joe Gilboy PA-C's video lessons you must be a member. Members can log in here or join now.
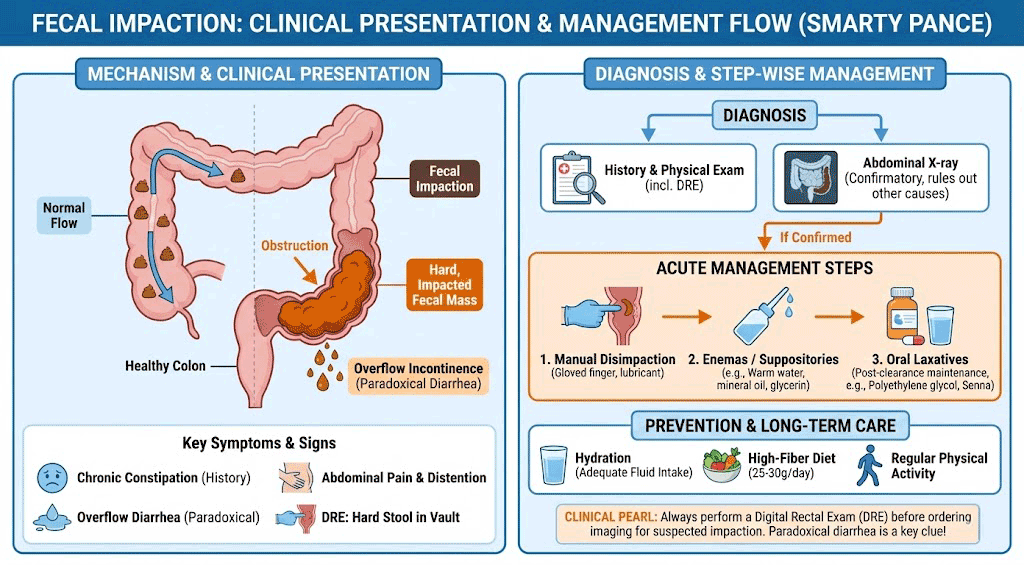
Fecal impaction is a large mass of hard, retained stool
- It generally occurs in the rectum but also may occur higher in the colon
- Complications include UTI, perforation of the colon, fecalith formation leading to appendicitis
Rock hard stool in the rectal vault on examination is diagnostic of distal impaction
- Abdominal plain film or CT will be confirmatory
- The elderly are at greater risk for developing chronic constipation
- Follow up colonoscopy to r/o colon CA

Abdominal X-ray done in the emergency room showing a huge fecal impaction extending from the pelvis upwards to the left subphrenic space and from the left towards the right flank, measuring over 40 cm in length and 33 cm in width.
Manual disimpaction digitally, followed by saline or tepid water enema for distal impaction
- More proximal impaction can be broken up by sigmoidoscopic water irrigation and suction
- Ensure the patient has sufficient fiber intake and hydration
Question 1 |
passing a nasogastric tube Hint: A nasogastric tube would not be used for an obstruction in the distal colon/rectum. | |
milk of magnesia Hint: Mechanical bowel obstruction in the rectum does not usually respond to oral laxatives. | |
opiate analgesics for pain Hint: One would avoid opiates in fecal impactions and other constipation problems because they tend to be more constipating. | |
oral sodium phosphate Hint: Mechanical bowel obstruction in the rectum does not usually respond to oral laxatives. | |
manual disimpaction |
References: Merck Manual · UpToDate