 Lecture
Lecture

51-year-old with rectal bleeding and abdominal pain
Patient will present as → a 45-year-old man with severe rectal pain when he defecates, which lasts for several hours and subsides until the next bowel movement. He has been constipated for the past 6 months, and when he does have a bowel movement, the stool is covered with bright red blood. A sentinel pile is noted on the physical exam.

To watch this and all of Joe-Gilboy PA-C's video lessons, you must be a member. Members can log in here or join now.
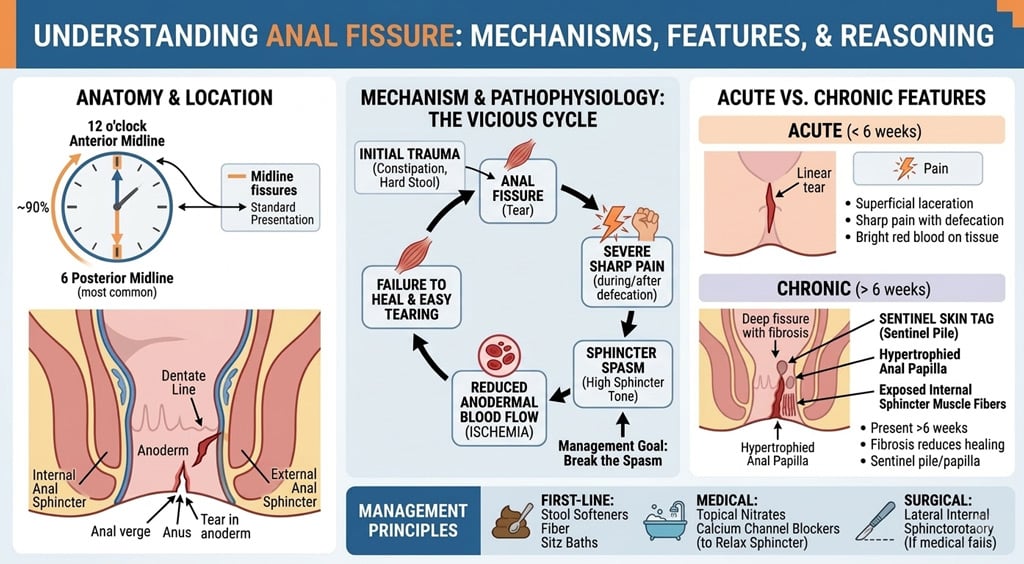
Anal fissures are believed to result from laceration by a hard or large stool or from frequent loose bowel movements
- Caused by: hard stool passage (constipation), hyperactive sphincter, disease process (e.g., Crohn’s disease)
- The fissure may cause internal sphincter spasm, decreasing blood supply and perpetuating the fissure
- Presents with pain in the anus, painful (can be excruciating) bowel movement, rectal bleeding, blood on toilet tissue after bowel movement, sentinel tag, tear in the anal skin, extremely painful rectal exam, sentinel pile, hypertrophic papilla

An anal fissure is a small tear in the thin, moist tissue (mucosa) that lines the anus. 90% of fissures are formed along the posterior midline of anal canal.
Diagnosis is made by history and visual inspection +/- anoscopy
- Alternatively, reproducing the patient's presenting complaints (ie, anal pain) by gentle digital palpation of the posterior (or anterior) midline anal verge is diagnostic
- A sentinel pile (thickened mucosa) is found below the fissure
- Unless findings suggest a specific cause or the appearance and/or location is unusual, further studies are not required
For patients with a typical anal fissure (ie, a single posterior or anterior fissure with no evidence of Crohn's disease), treatment consists of a combination of supportive measures (fiber, sitz bath, topical analgesic) and one of the topical vasodilators (nifedipine or nitroglycerin) for one month.
Treatment acronym WASH
- W arm sitz baths: which can relax the anal sphincter and improve blood flow to the anal mucosa, are recommended for patients with anal fissures
- During a sitz bath, the anus is immersed in warm water for approximately 10 to 15 minutes two to three times daily or showers immediately after every bowel movement
- A nalgesics: 2% lidocaine jelly
- Topical vasodilator:
- topical 0.4% nitroglycerin rectal ointment (Rectiv) twice daily
- topical 0.2 to 0.3% nifedipine ointment two to four times daily in patients who have access to a compounding pharmacy
- Topical vasodilator:
- S tool softeners (Colace)
- H igh Fiber: the recommended dietary fiber intake is between 20 and 35 grams per day
- Patients who continue to have difficulty with hard bowel movements despite increasing dietary fiber intake may use fiber supplements, such as psyllium seed (Metamucil), methylcellulose (Citrucel), wheat dextrin (Benefiber), and calcium polycarbophil (Fibercon)
Second-line therapy
- Topical Ca channel blocker (Diltiazem 2% rectal gel is applied three times daily for eight weeks), or botulinum toxin type A injection
Question 1 |
Anal fissure | |
Crohn’s disease Hint: Other symptoms would be abdominal pain and prolonged diarrhea. It causes fissures outside the midline. 50% of fissures are painless. | |
Anal carcinoma Hint: Atypical and shape of fissure. History of human papillomavirus infection. | |
Tuberculosis Hint: History of tuberculosis. Lateral site of fissure. |
Question 2 |
Lateral anal sphincterotomy. | |
Cryosurgery. Hint: Is used in treating hemorrhoids | |
Infrared coagulation. Hint: Is used in treating hemorrhoids | |
Temporary Thiersch operation. Hint: Is used in treating rectal prolapsed. |
Question 3 |
Topical diltiazem Hint: It heals about 65% of fissures with very few side-effects. It heals most fissures that do not heal with GTN. | |
Topical glyceryl trinitrate (GTN) ointment Hint: reduces the maximum resting anal pressure of the order of 35%. It relaxes the internal anal sphincter, (via the release of the neurotransmitter nitric oxide) thereby improving the blood supply to the mucosa and ischaemic fissure and leads to its healing in about 60% of patients in 8 weeks. | |
Botulinum toxin Hint: It is an exotoxin produced by CI. Botulinum and is a potent neurotoxin. It reduces the myogenic tone and adrenaline-mediated contractile response to sympathetic stimulation of the internal anal sphincter thereby reducing the resting anal pressure, usually by about 25%. | |
Cisapride |
Question 4 |
Anterior fissures account for about 90% of those encountered in women. | |
Most commonly occur at the posterior midline. Hint: See A for explanation | |
Anal advancement flap is a form of treatment. Hint: See A for explanation | |
May be due to trauma caused by the strained evacuation of a hard stool. Hint: See A for explanation |
Question 5 |
Sitz baths Hint: See E for explanation | |
Topical nitroglycerin ointment Hint: See E for explanation | |
Topical silver nitrate Hint: See E for explanation | |
Fiber supplementation Hint: See E for explanation | |
all of the above |
|
List |
References: Merck Manual · UpToDate