 Lecture
Lecture
Patient with celiac disease will present as → a 34-year-old male presents to the clinic with a six-month history of chronic diarrhea, weight loss, and generalized weakness. He reports frequent abdominal pain and bloating after meals. He has also noticed a blistering, itchy rash on his elbows and knees. His medical history is significant for iron deficiency anemia. Physical examination reveals pallor, a distended abdomen, and a rash consistent with dermatitis herpetiformis. Laboratory tests show low hemoglobin and hematocrit levels, elevated transaminases, and a positive tissue transglutaminase (tTG) IgA antibody. Given his clinical presentation and positive serologic test for celiac disease, the patient is diagnosed with celiac disease. Upper endoscopy with a biopsy of the small intestine is scheduled to confirm villous atrophy. He is started on a strict gluten-free diet and referred to a dietitian for comprehensive dietary education and management. He is also advised to avoid foods that may contain hidden sources of gluten and to be aware of cross-contamination. Follow-up is planned to monitor his response to the gluten-free diet, check for improvement in symptoms, and reassess his nutritional status.
Patient with non-celiac gluten intolerance will present as → a 28-year-old female presents to the clinic with a one-year history of recurrent abdominal bloating, diarrhea, and fatigue. She notes that her symptoms tend to worsen after consuming foods containing gluten, such as bread, pasta, and pastries, but she does not experience any symptoms when she avoids gluten. She has tried a gluten-free diet for several weeks, which seemed to improve her symptoms. Her medical history is unremarkable, and she denies any weight loss, anemia, or skin rashes. Physical examination and routine laboratory tests, including a celiac panel, are all normal. Based on her history of symptoms improving with a gluten-free diet and the absence of diagnostic markers for celiac disease, the patient is diagnosed with non-celiac gluten intolerance. She is advised to continue a gluten-free diet and to monitor her symptoms closely. She is also educated on reading food labels and avoiding cross-contamination. A referral to a dietitian is made to ensure she maintains a balanced and nutritious diet while avoiding gluten. Follow-up appointments are scheduled to monitor her symptoms and nutritional status.

To watch this and all of Joe-Gilboy PA-C's video lessons you must be a member. Members can log in here or join now.
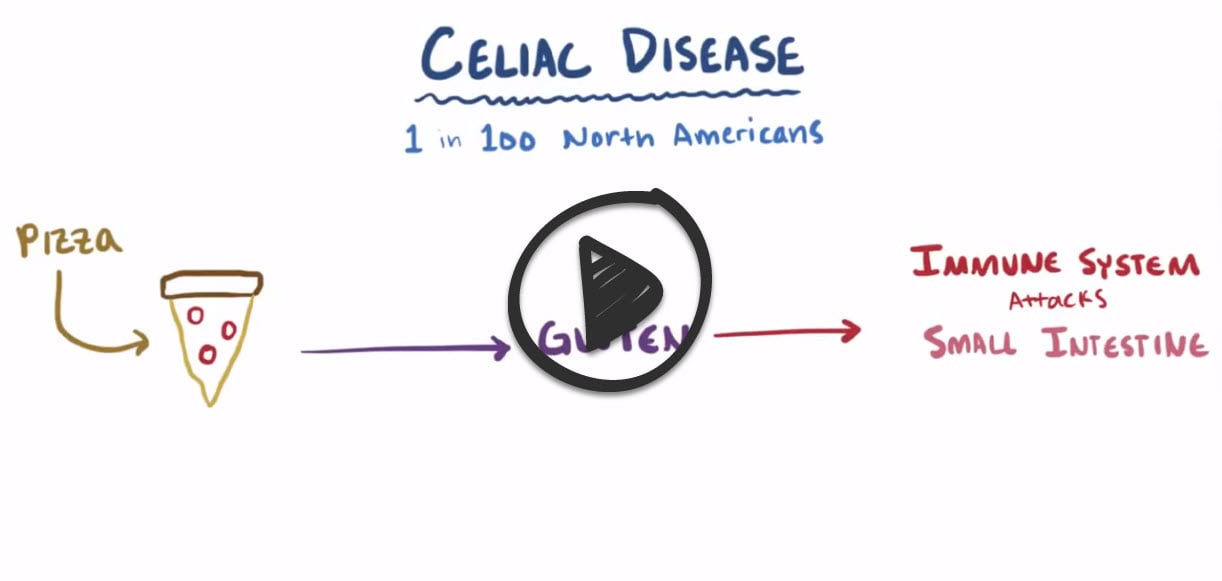
Celiac Disease is an autoimmune disorder where gluten intake damages the small intestine, leading to nutrient absorption issues and symptoms like diarrhea, abdominal pain, and fatigue. Diagnosis is through blood tests and intestinal biopsy. Treatment requires a strict, lifelong gluten-free diet.
Celiac disease is characterized by small bowel inflammation secondary to ingesting gluten-containing foods such as wheat, rye, and barley, leading to malabsorption.
- Celiac disease is an autoimmune disorder in individuals with HLA-DQ2 or HLA-DQ8
- Celiac disease runs in families
- People with a first-degree relative with celiac disease (parent, child, sibling) have a 1 in 10 risk of developing celiac disease.
- 1:300 in southwest Ireland
- >1:5000 in North America
- People with a first-degree relative with celiac disease (parent, child, sibling) have a 1 in 10 risk of developing celiac disease.
Clinical presentation is variable and may lead to a delay in diagnosis in milder cases
- Diarrhea, bloating, steatorrhea, weight loss, fatigue, and signs of nutrient deficiencies (e.g., iron, folate, calcium)
- Dermatitis herpetiformis (pruritic papulovesicular rash) is a classic extraintestinal manifestation
- Infants and children may present with failure to thrive
Non-Celiac Gluten Sensitivity (NCGS): A condition causing symptoms similar to celiac disease, such as bloating and abdominal pain, WITHOUT the autoimmune intestinal damage. Diagnosed by ruling out celiac disease and wheat allergy, and observing symptom improvement on a gluten-free diet. Gluten sensitivity levels vary, and some individuals may tolerate minimal gluten.
- NCGS does not involve autoimmune damage to the intestine
- Normal serum biomarkers - NCGS is diagnosed by ruling out celiac disease and wheat allergy and observing symptom improvement on a gluten-free diet.
- Individuals with NCGS may have varying levels of sensitivity and may be able to tolerate small amounts of gluten.
Celiac Disease and Non-Celiac Gluten Sensitivity/Intolerance (NCGS):
| Aspect | Celiac Disease | Non-Celiac Gluten Sensitivity (NCGS) |
| Cause | An autoimmune disorder where the ingestion of gluten leads to damage in the small intestine. | Sensitivity to gluten without autoimmune damage to the small intestine. |
| Immune Response | Autoimmune response leading to damage of the villi in the small intestine. | No autoimmune response or damage to the small intestine. |
| Symptoms | Diarrhea, abdominal pain, bloating, weight loss, anemia, fatigue, and more. Can lead to serious complications if untreated. | Similar gastrointestinal symptoms (e.g., bloating, pain), and extraintestinal symptoms (e.g., headache, fatigue) without the autoimmune complications. |
| Diagnosis | Blood tests for specific antibodies, confirmed by biopsy of the small intestine. | Diagnosis by exclusion (ruling out celiac disease and wheat allergy) and improvement of symptoms on a gluten-free diet. |
| Treatment | Strict, lifelong gluten-free diet. | Gluten-free diet, but sensitivity levels vary; some individuals may tolerate small amounts of gluten. |
| Nutrient Absorption | Impaired due to damage of the villi, leading to potential nutrient deficiencies. | Not directly affected, as there is no damage to the villi. |
| Long-term Complications | Untreated celiac disease can lead to serious health complications, including osteoporosis, infertility, neurological conditions, and increased risk of some cancers. | Not typically associated with the long-term complications seen in untreated celiac disease, but quality of life can be significantly affected. |
IgA endomysial antibody (EMA) and anti-tissue transglutaminase (anti-tTG) antibodies. If the serologic tests are positive, an upper endoscopy with a small bowel biopsy is performed to confirm the diagnosis. Testing for celiac disease should ideally be performed while patients are on a gluten-containing diet.
- Tissue Transglutaminase Antibodies (tTG-IgA): The tTG-IgA test will be positive in about 98% of patients with celiac disease who are on a gluten-containing diet.
- IgA Endomysial antibody (EMA-IgA): The EMA test has a specificity of almost 100% but is not as sensitive as the TTG-IgA test. About 5-10% of people with celiac disease do not have a positive EMA test.

"Endoscopic intestinal mucosal biopsy of the proximal duodenum (bulb) and distal duodenum is the standard method for confirmation of the diagnosis in patients with a positive serologic test (IgA endomysial antibody) for celiac disease."
Treat celiac disease with a gluten-free diet. Supplementation may be needed to correct nutritional deficiencies in iron, vitamin B12, folic acid, calcium, and vitamin D.
- Patients are encouraged to consult a dietitian and join a celiac support group such as Beyond Celiac or the Celiac Disease Foundation.
Non-Celiac Gluten Sensitivity (NCGS) is also treated with a gluten-free diet, but sensitivity levels vary; some individuals may tolerate small amounts of gluten.
 Osmosis Osmosis |
|
 |
Celiac disease is characterized by symptoms of dermatitis herpetiformis, steatorrhea, decreased bone density, failure to thrive, anemia, and weight loss. There is a strong association of this disease with HLA-DQ8 and HLA-DQ2, and it has a higher prevalence in patients of northern European descent.
Play Video + QuizCeliac Disease Diagnosis and Treatment

Celiac disease is easily diagnosed with a plethora of biopsy and serological findings. On biopsy, patients will display blunting of the intestinal villi, and increased lymphocyte infiltration of the lamina propria. Serology will show an immune response, which produces anti-endomysial antibodies, anti-gliadin antibodies, and anti-tissue transglutaminase antibodies. Treatment of celiac disease begins with lifestyle modifications. Patients should adhere to a gluten-free diet, and in cases that do not resolve, glucocorticoids can be added. Refractory cases of skin manifestations, known as dermatitis herpetiformis can be treated with Dapsone.
Play Video + QuizQuestion 1 |
Lactase deficiency Hint: Lactase deficiency manifests as bloating, flatus, and abdominal cramping after ingestion of milk and milk based product. | |
Impaired absorption of fat Hint: Impaired absorption of fat causes steatorrhea and is seen in pancreatic and gallbladder/bile duct lesions. | |
Impaired absorption of Vitamin B12 Hint: Vitamin B12 deficiency manifests by fatigue, smooth, thick and red tongue. It’s seen in pernicious anemia. | |
Sensitivity to gliadin |
Question 2 |
Type 0 Hint: Type 0: pre-infiltrative stage (normal). | |
Type 1 | |
Type 2 Hint: Type 2: hyperplastic lesion (type 1 plus hyperplastic crypts). | |
Type 3 Hint: Type 3: destructive lesion (type 2 plus atrophy of progressively more severe degrees [termed 3a, 3b, and 3c]. |
Question 3 |
Dermatitis herpetiformis Hint: Dermatitis herpetiformis is regarded as a cutaneous variant of celiac disease. It is a characteristic skin rash consisting of pruritic papulovesicles over the extensor surfaces of the extremities and over the trunk, scalp, and neck. Dermatitis herpetiformis occurs in <10% of patients with celiac disease. | |
Aphthous ulcers Hint: Present in children and adults with celiac disease. It is neither characteristic nor specific for celiac disease. However, ulcers often regress once the patients are on a gluten-free diet. | |
Iron-deficiency anemia Hint: Iron deficiency anemia is a very common extraintestinal manifestation of celiac disease. | |
Conjunctivitis |
Question 4 |
Endoscopic mucosal biopsy of the small intestine. | |
Antigliadin antibodies Hint: Antigliadin antibodies are not recommended because of their lower sensitivity and specificity. | |
IgA tissue transglutaminase antibodies Hint: Is a serologic screening test that has a 95% sensitivity and 95% specificity for celiac disease. | |
IgA antiendomysial antibodies Hint: Is a serologic screening test. |
Question 5 |
IgA tissue transglutaminase antibody is a serologic screening test for celiac disease. Hint: See D for explanation | |
Intestinal symptoms in children include diarrhea, weight loss, abdominal distension, failure to thrive. Hint: See D for explanation | |
Gluten-free diet is essential in the treatment of patients with celiac disease. Hint: See D for explanation | |
Prednisolone has no role in the management of celiac disease. |
|
List |
References: Merck Manual · UpToDate