

2 y/o with tachypnea, hypoxemia, and fever
Patient will present as → a 9-month-old infant presents with a three-day history of a mild respiratory tract infection with serous nasal discharge, fever of 38.5 C (101.4 F), and decreased appetite. Physical exam reveals a tachypneic infant with audible wheezing and a respiratory rate of 65. Flaring of the alae nasi, use of accessory muscles, and subcostal and intercostal retractions are noted. Expiratory wheezes are present.
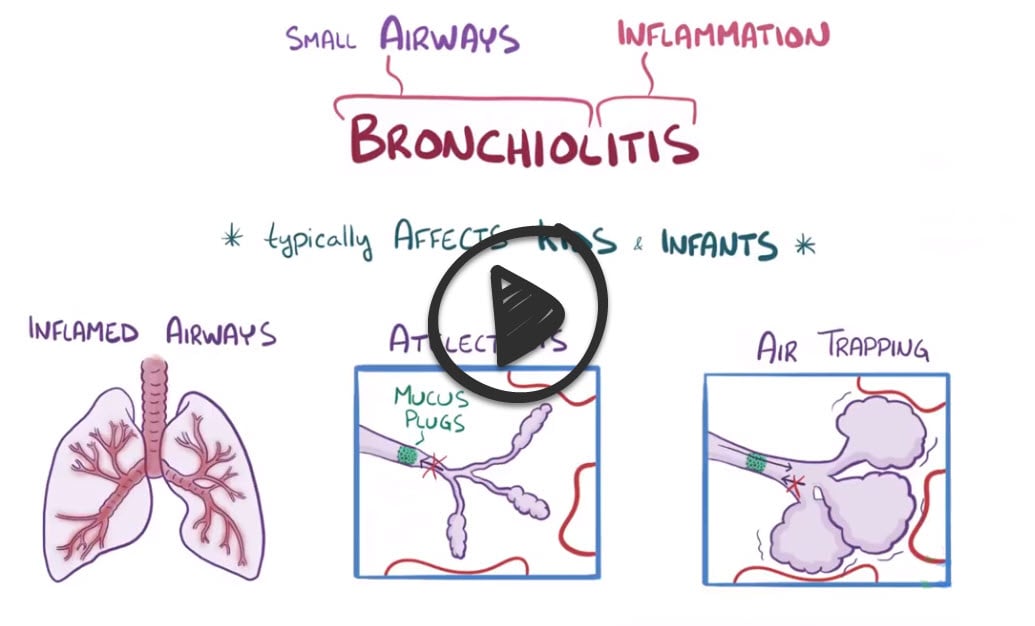
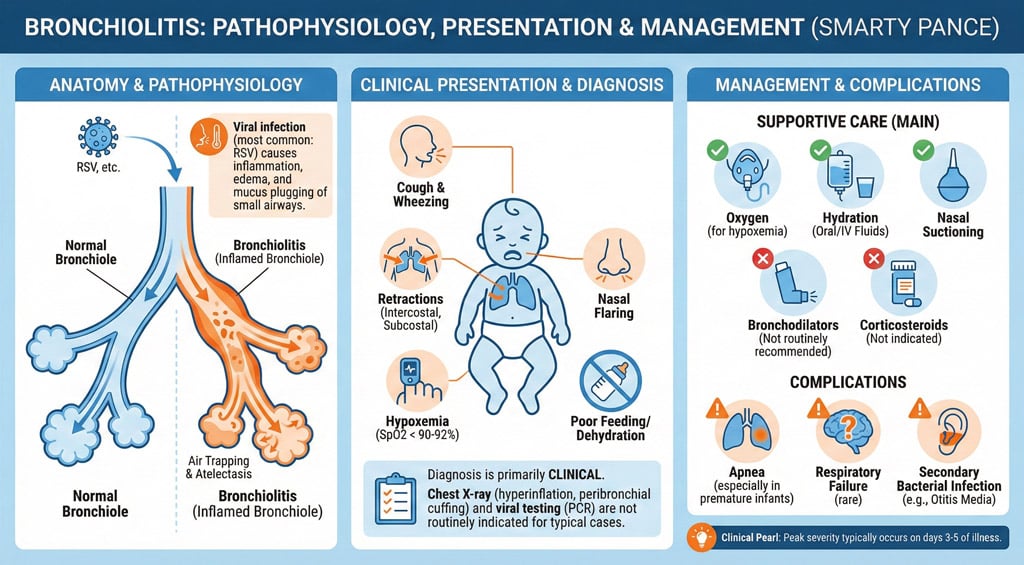 Bronchiolitis is inflammation of the bronchioles, the smallest air passages of the lungs, which usually occurs in children less than two years of age
Bronchiolitis is inflammation of the bronchioles, the smallest air passages of the lungs, which usually occurs in children less than two years of age
- Respiratory syncytial virus (RSV) is the most common cause of acute bronchiolitis
- It is most common in the fall and winter months. CXR is often normal, but may show air trapping and peribronchial thickening
- Diagnosed with nasal washing for RSV culture and antigen assay
- Hospitalization if O2 < 95%, age < 3 months, respiratory rate > 70 or atelectasis on chest radiograph
Diagnosis is clinical—based on history and physical exam; routine chest X-ray or viral testing is not required unless diagnosis is unclear
- Viral testing (if needed) is done by nasal wash/swab for RSV antigen or PCR (PCR = most sensitive)
- CXR (not routine) may show hyperinflation, perihilar infiltrates, increased interstitial markings, or patchy atelectasis

A CXR of a child with bronchiolitis showing the typical bilateral perihilar fullness (arrows)
The mainstay of treatment for bronchiolitis is supportive care—nasal suctioning, use of a humidifier, hydration, and antipyretics (e.g., acetaminophen or ibuprofen)
- Patients with hурохеmiа should receive supplemental οxygen by nasal cannula, face mask, or hood
- Variable thresholds are used for starting oxygen therapy in infants with bronchiolitis, most commonly SpO2 <90 to <92 percent
- The only treatment demonstrated to improve bronchiolitis is oxygen
- Bronchodilators (e.g., albuterol via nebulizer) are not recommended — the 2014 AAP guideline advises against routine bronchodilator use in bronchiolitis
- Systemic steroids are generally not recommended in bronchiolitis except in cases with bronchial reactivity (e.g., RSV-induced wheezing) or coexisting asthma.
- Symptoms of bronchiolitis typically peak at days 3-5 of illness and resolve within 7-10 days, though a cough may persist for weeks
- Ribavirin is reserved for severe cases involving high-risk populations, such as patients with underlying lung or heart disease or immunocompromised states
- RSV vaccines are primarily indicated in specific populations, such as adults over 60 years or high-risk infants (current CDC guidelines)
- Nirsevimab (a long-acting anti-RSV monoclonal antibody, single dose) is recommended for ALL infants <8 months born during or entering their first RSV season (ACIP 2023) — it has largely replaced palivizumab
- Maternal RSV vaccine (RSVpreF / Abrysvo) given in pregnancy at 32–36 weeks is an alternative pathway — if the birthing parent was vaccinated ≥14 days before delivery, the infant generally does not also need nirsevimab
- A second-season dose is given to high-risk infants 8–19 months (e.g., chronic lung disease of prematurity, severe immunocompromise)
- Palivizumab (monthly ×5 during RSV season) is now largely superseded by nirsevimab, reserved for limited situations where nirsevimab is unavailable
- Severe Respiratory Distress: Marked by significant tachypnea (>60–70 breaths/min), nasal flaring, grunting, or intercostal/subcostal retractions
- Hypoxemia: SpO₂ <90% on room air (persistent, not brief dips)
- Apnea: Especially in infants <2 months or with history of prematurity
- Dehydration or Poor Feeding: Inability to maintain adequate oral intake due to respiratory effort or lethargy
- Worsening Clinical Status: Persistent or worsening symptoms despite outpatient management
- High-Risk Groups: Infants <3 months, preterm infants, or those with underlying conditions (e.g., congenital heart disease, chronic lung disease, or immunodeficiency)
- Social Factors: Lack of reliable caregiver support, limited access to follow-up care, or unsafe home environment
Management of Bronchiolitis by Severity
| Severity | Clinical Features | Setting | Key Interventions |
| Mild | Minimal distress, normal feeding, SpO₂ ≥90% | Outpatient | Supportive care at home: nasal suctioning, hydration, antipyretics if needed |
| Moderate | Tachypnea, mild–moderate retractions, transient SpO₂ dips <90% (not sustained) | Inpatient | Supportive care, nasal suctioning, IV/NG fluids if poor intake, oxygen only if SpO₂ remains <90% |
| Severe | Persistent SpO₂ <90%, marked retractions, nasal flaring, apnea, lethargy | Hospital (often PICU) | Escalating O₂ (low flow → HFNC → CPAP/BPAP), IV/NG fluids, close monitoring, intubation if respiratory failure |
 Osmosis Osmosis |
|
 |
Question 1 |
Which of the following is the most common etiological agent of acute bronchiolitis in infants and young children?
Streptococcus pneumoniae Hint: This is not the most common cause | |
Mycoplasma pneumoniae Hint: This is not the most common cause | |
Parainfluenza virus Hint: This is not the most common cause | |
Respiratory syncytial virus (RSV) | |
Adenovirus Hint: This is not the most common cause |
Question 2 |
Chest X-ray Hint: May be used to rule out pneumonia but is not necessary for the initial diagnosis of bronchiolitis. | |
Nasopharyngeal swab for viral PCR | |
Complete blood count (CBC) Hint: Not specific for diagnosing bronchiolitis and typically shows nonspecific findings. | |
Pulmonary function tests Hint: Not feasible or practical in infants with acute respiratory distress. | |
Blood culture Hint: Indicated if there is a suspicion of bacterial sepsis, not for uncomplicated bronchiolitis. |
Question 3 |
Oral corticosteroids Hint: Not recommended for the treatment of bronchiolitis as they have not been shown to improve outcomes. | |
Antibiotic therapy Hint: Not indicated unless there is a clear evidence of bacterial co-infection, which is uncommon in uncomplicated bronchiolitis. | |
Supportive care, including hydration and nasal suctioning | |
Nebulized albuterol treatments Hint: May be trialed in some cases, but evidence does not consistently show benefit in bronchiolitis. | |
Hospitalization and oxygen therapy
Hint: Indicated for severe cases with significant respiratory distress or hypoxemia, not mild cases. |
Question 4 |
Respiratory rate > 70 breaths per minute Hint: A respiratory rate greater than 70 breaths per minute indicates significant respiratory distress and is a criterion for hospitalization to provide appropriate respiratory support and monitoring. | |
Temperature > 100.5°F (38°C) | |
Oxygen saturation (SpO2) < 95% on room air Hint: Infants with bronchiolitis showing an oxygen saturation less than 95% on room air may require supplemental oxygen, monitoring, and possibly further intervention, making this an indication for hospitalization. | |
Apnea Hint: Episodes of apnea in infants with bronchiolitis are a critical concern, especially in young infants or those with a history of prematurity. This condition requires immediate hospitalization for continuous monitoring and intervention. | |
Poor feeding and/or dehydration Hint: Difficulty feeding leading to dehydration is a common complication of bronchiolitis in infants that may necessitate hospitalization for fluid management and supportive care. |
|
List |
References: Merck Manual · UpToDate