The NCCPA™ PANCE Pulmonary Content Blueprint other pulmonary diseases
| Bronchiectasis | Patient will present as → a 25-year-old cystic fibrosis patient complaining of chronic, frequent coughing productive of yellow and green sputum. She recently recovered from a Pseudomonas spp. Pneumonia requiring hospitalization. On physical examination, you notice foul breath, purulent sputum, and hemoptysis, along with a CXR demonstrating dilated and thickened airways with “plate-like” atelectasis (scarring). A condition in which the lungs' airways become dilated and damaged, leading to inadequate clearance of mucus in airways
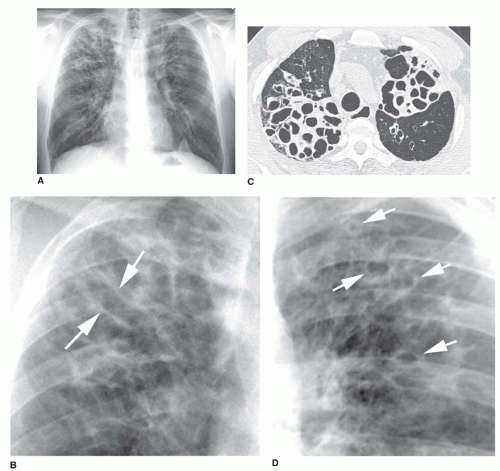
DX: CXR = linear “tram track” lung markings, dilated and thickened airways – “plate-like” atelectasis
TX: ambulatory oxygen, aggressive antibiotics for acute exacerbations, CPT (chest physiotherapy = bang on the back); eventual lung transplant  Chest X-ray of hyperinflated lung with bronchiectasis at the right upper lobe of a 12-year-old boy.  A CT scan demonstrating very pronounced bronchiectasis in a 75-year-old man, especially on the right (left in the picture). There is a florid superinfection with a large accompanying effusion |
{kind=link}
{kind=link}