 Lecture
Lecture
Patient will present as → a 25-year-old cystic fibrosis patient complaining of chronic, frequent coughing productive of yellow and green sputum. She recently recovered from a Pseudomonas spp. Pneumonia requiring hospitalization. On physical examination, you notice foul breath, purulent sputum, and hemoptysis, along with a CXR demonstrating dilated and thickened airways with “plate-like” atelectasis (scarring).

To watch this and all of Joe-Gilboy PA-C's video lessons you must be a member. Members can log in here or join now.
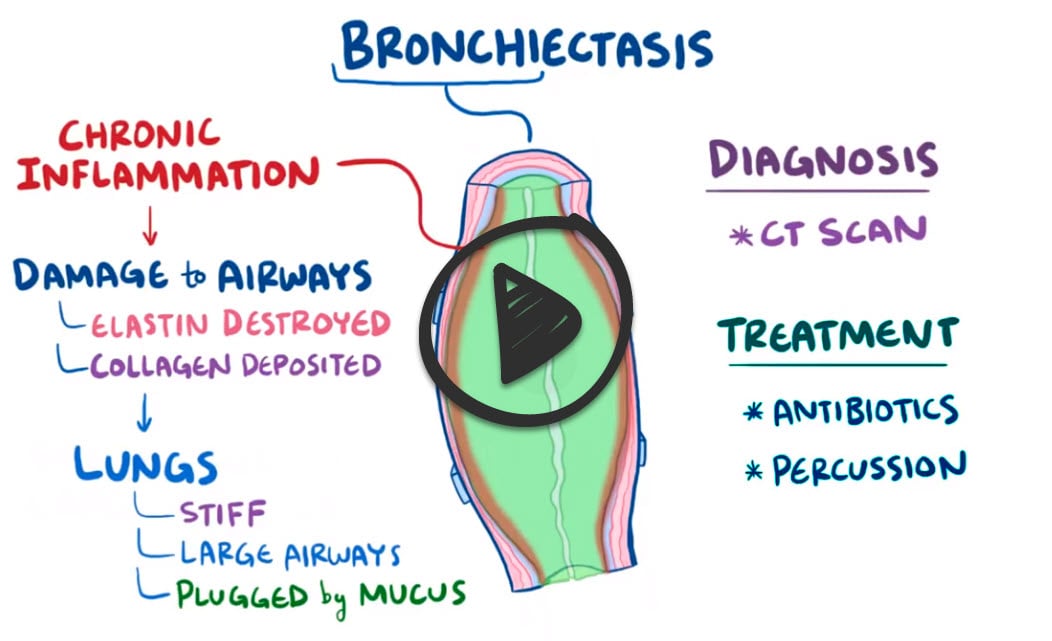
Bronchiectasis is described as the permanent dilation or destruction of the bronchial walls
- The most widely accepted model describes a "vicious cycle" of inflammation => airway destruction => abnormal mucus clearance, and infection or colonization by bacteria
- Bronchiectasis is best considered the common endpoint of various disorders that cause chronic airway inflammation
- The dilation and destruction of larger bronchi is caused by chronic infection and inflammation. Common causes of this inflammation are cystic fibrosis, immune defects, recurrent infections, and foreign body aspirations. Some cases are idiopathic
- The most common cause is cystic fibrosis
- Presents as chronic cough, purulent sputum, fever, weakness, weight loss, dyspnea in some patients, and hemoptysis
- Hemoptysis is generally mild, originates from bronchial arteries, and is seen in 50% to 70% of all cases
- The main causative agents of bronchiectasis are adenovirus and influenza
- Bacterial causes: There is little common consensus but Streptococcus pneumoniae and Pseudomonas aeruginosa are the most commonly isolated bacteria
- Colonization with P. aeruginosa tends to indicate severe disease and predicts worse outcomes
CXR – linear ("tram track") lung markings, atelectasis, dilated and thickened airways, “Plate-like” atelectasis (scarring)
- The gold standard diagnosis is a CT of the chest - findings include abnormally widened and thickened airways with irregular walls and lack of tapering

Chest X-ray of hyperinflated lung with bronchiectasis at the right upper lobe of a 12-year-old boy.

A CT scan demonstrating very pronounced bronchiectasis in a 75-year-old man, especially on the right (left in the picture). There is a florid superinfection with a large accompanying effusion
Aggressive antibiotics are the mainstay of treatment
- Chest physiotherapy, nutritional support, inhalable indomethacin (shown to decrease bronchial hypersecretion by inhibiting neutrophil recruitment), bronchodilators, supplemental oxygen, immunoglobulin administration for immunoglobulin deficiency, replacement treatment for patients with alpha-1-anti-trypsin deficiency, and recombinant DNAase to reduce sputum viscosity in patients with cystic fibrosis (CF)
- Eventually lung transplant
 Osmosis Osmosis |
|
 |

Bronchiectasis is an obstructive lung disease caused by bronchial obstruction or chronic necrotizing infection. The subsequent muscle and elastic tissue damage permanently dilates the airways, which may trap air in the lungs and lead to collapse of the bronchioles. Common symptoms include increased purulent sputum production and hemoptysis. Bronchiectasis is associated with poor ciliary motility, a result of congenital causes like Kartagener’s Syndrome, or acquired causes like smoking. Other predisposing conditions are cystic fibrosis, which impairs clearance of mucus from the airways, and allergic bronchopulmonary aspergillosis (APBA), an immune response to Aspergillus fungus.
Play Video + QuizQuestion 1 |
Acute bronchitis Hint: Barring underlying pulmonary pathology,the chest x-ray in acute bronchitis should be normal. | |
Bronchiectasis | |
Pneumonia Hint: While the history may suggest pneumonia, the radiographic findings do not support this diagnosis. | |
Tuberculosis Hint: Tuberculosis would present with cavitating granuloma formation more commonly at the apices. |
Question 2 |
Bronchiectasis | |
Tuberculosis Hint: TB would present with CXR findings in the apical or posterior segments of the upper lobes. | |
Adenocarcinoma Hint: Radiographic findings of adenocarcinoma include enlarged nodule or mass; persistent opacity, atelectasis or pleural effusion. The sputum would not likely be foul smelling. | |
Pulmonary fibrosis Hint: Pulmonary fibrosis does not present with dilated bronchi or ring-like markings on CXR |
|
List |
References: Merck Manual · UpToDate