The NCCPA™ PANCE Pulmonary Content Blueprint covers nine topics under the label infectious disorders, including four types of pneumonia.
| Condition | Classic Presentation | Diagnostics & Next Steps |
|---|---|---|
| Acute Bronchiolitis (RSV) | Viral prodrome in infants <= 2 years progressing to diffuse wheezing, tachypnea, and respiratory distress. | Clinical diagnosis emphasizing supportive care with nasal suctioning and supplemental O2 if sats <= 90%. |
| Acute Bronchitis | Cough persisting >= 5 days up to 3 weeks with normal vital signs and clear lung fields. | Clinical diagnosis requiring patient education to avoid antibiotics and focus entirely on symptomatic relief. |
| Acute Epiglottitis | Rapid onset of dysphagia, drooling, and distress (3 Ds) in an unimmunized child assuming a tripod sniffing position. | Secure the airway immediately in the OR followed by IV ceftriaxone and a lateral neck film showing a thumbprint sign. |
| Croup | Parainfluenza virus causing a barking seal-like cough and inspiratory stridor in children 6 months to 3 years. | Administer dexamethasone for all cases and add nebulized racemic epinephrine for stridor at rest alongside a PA neck X-ray showing a steeple sign. |
| Influenza | Abrupt onset of high fever >= 100.4 F, severe myalgias, and headache during winter months. | Diagnose with rapid antigen or PCR and start oseltamivir if within 48 hours of onset or for high-risk patients. |
| Pertussis (Whooping Cough) | Severe paroxysmal coughing fits ending in an inspiratory whoop and often post-tussive emesis. | Confirm with nasopharyngeal PCR and treat with a macrolide (azithromycin) to reduce bacterial transmission. |
| Pneumonia | Fever, productive cough, and focal lung exam findings like localized crackles, dullness to percussion, or egophony. | Order a PA and lateral CXR looking for lobar or interstitial infiltrates and initiate empiric antibiotics based on the clinical setting. |
| Tuberculosis | Chronic cough, night sweats, weight loss, and hemoptysis in a patient with known exposure risk or travel history. | Screen with IGRA or PPD (PPD rules) and confirm with apical cavitary lesions on CXR followed by acid-fast bacilli smear and culture. |
| Acute bronchiolitis (ReelDx) | ReelDx Rotation Room (bronchiolitis)Patient will present as → a 9-month-old infant with a three-day history of a mild respiratory tract infection with serous nasal discharge, fever of 38.5 C (101.4 F), and decreased appetite. Physical exam reveals a tachypneic infant with audible wheezing and a respiratory rate of 65. Flaring of the alae nasi, use of accessory muscles, and subcostal and intercostal retractions are noted. Expiratory wheezes are present. Most often caused by RSV - commonly in the fall and winter months
DX: Clinical DX (URI prodrome → wheezing/crackles + ↑ work of breathing); if needed → nasopharyngeal PCR; CXR NOT routine (if done: hyperinflation, peribronchial thickening) TX: TX: Supportive care—oxygen, hydration, nasal suctioning
Vaccination (view current CDC guidelines)
|
||||||||||||||||||||||||||||||||||||
| Acute bronchitis (ReelDx) | Patient will present as → a 23-year-old female with a one-week history of cough productive of whitish sputum. This was preceded one week prior by a URI. She denies chills, night sweats, shortness of breath, or wheezing. Temperature is 99.9°F (37.7°C). 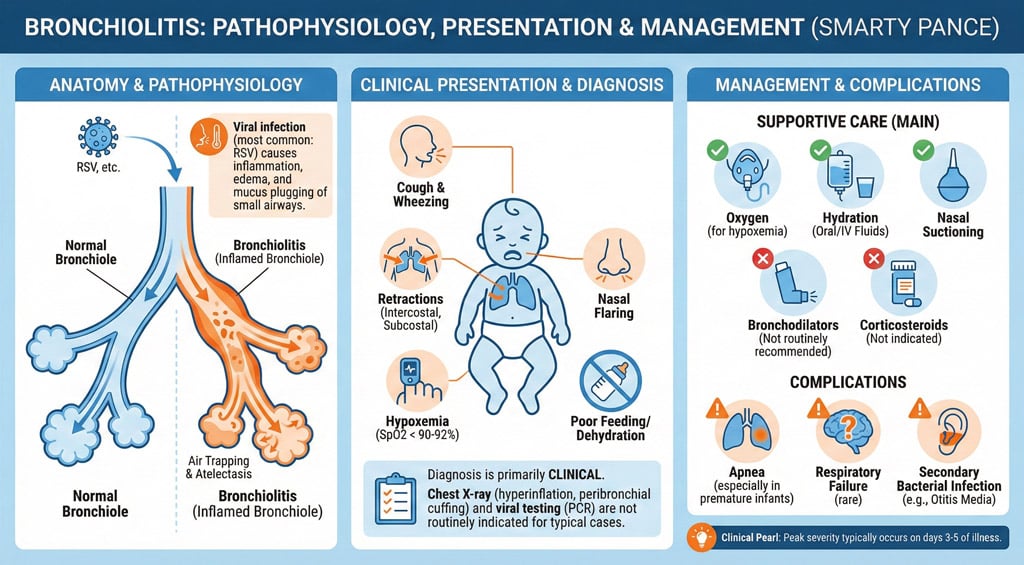 Acute bronchitis is defined by a cough >5 days; it can last 1-3 weeks Acute bronchitis is defined by a cough >5 days; it can last 1-3 weeks
Organisms:
Presentation:
DX: Obtain CXR if the diagnosis is uncertain or symptoms persist despite conservative treatment TX: symptomatic and supportive - hydration, expectorant, analgesic, B2 agonist, cough suppressant
|
||||||||||||||||||||||||||||||||||||
| Acute epiglottitis | Patient will present as → a 3-year-old boy who is brought to the ER with a sudden onset of fever (104.0 F), respiratory distress, and stridor. On examination, the boy appears acutely ill. He is sitting, leaning forward with his mouth open. He has a muffled voice and is drooling. When asked, the parents report, “We don’t believe in vaccinations.” Supraglottic inflammation and obstruction of the airway due to infection with Haemophilus influenzae type B (Hib)
Tripod positioning ⇒ 3 Ds of epiglottitis:
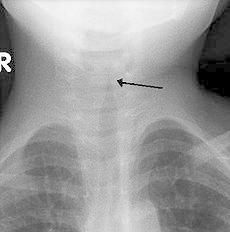
DX: lateral neck X-ray, which will classically show a thumbprint sign from swelling of the epiglottis. Secure airway, then culture for H.flu
TX: Treatment involves intubating if necessary, supportive care, and ceftriaxone. May be treated as an outpatient if stable  The lateral soft-tissue radiograph reveals the "thumb sign" that indicates a swollen epiglottis, suggestive of epiglottitis. |
||||||||||||||||||||||||||||||||||||
| Croup (ReelDx) | Patient will present as → a 2-year-old boy who is brought to you by his father, who is concerned about a “barking cough,” mild fever, and a hoarse voice. He reports that he had a runny nose last week that has since resolved. Physical exam reveals inspiratory stridor. AP neck film is shown here. Croup refers to an infection of the upper airway, which obstructs breathing and causes a characteristic barking cough
Treatment:
 AP x-ray of the neck in a child with croup demonstrating the steeple sign (narrowing of the trachea) |
||||||||||||||||||||||||||||||||||||
| Influenza (ReelDx) | Patient will present as → a 5-year-old with sudden onset of fever, chills, malaise, sore throat, headache, and coryza. The child is also complaining of myalgia, especially in her back and legs. On physical exam, the patient appears lethargic, has a temperature of 102.5 F, and palpable cervical lymph nodes. Breath sounds are distant with faint end-expiratory wheezes. Influenza is a viral respiratory infection caused by orthomyxovirus resulting in fever, coryza, cough, headache, and malaise
Vaccination
Dx: rapid antigen test in the clinic, rapid serology test more accurate
Treatment is symptomatic (for most) or with antivirals ⇒ ideally< 48 hours – Tamiflu (oseltamivir), inhaled Relenza (zanamivir), IV Rapivab (peramivir), and oral baloxavir (Xofluza)
 Chest X-ray in a patient with viral pneumonia demonstrating diffuse bilateral infiltrates. |
||||||||||||||||||||||||||||||||||||
| Pertussis (Whooping Cough) | Patient will present as → a 4-year-old boy with a severe cough following one week of cold symptoms, including sneezing, conjunctivitis, and nocturnal cough. He presents with paroxysms of cough followed by deep inspiration and occasional post-tussive emesis. 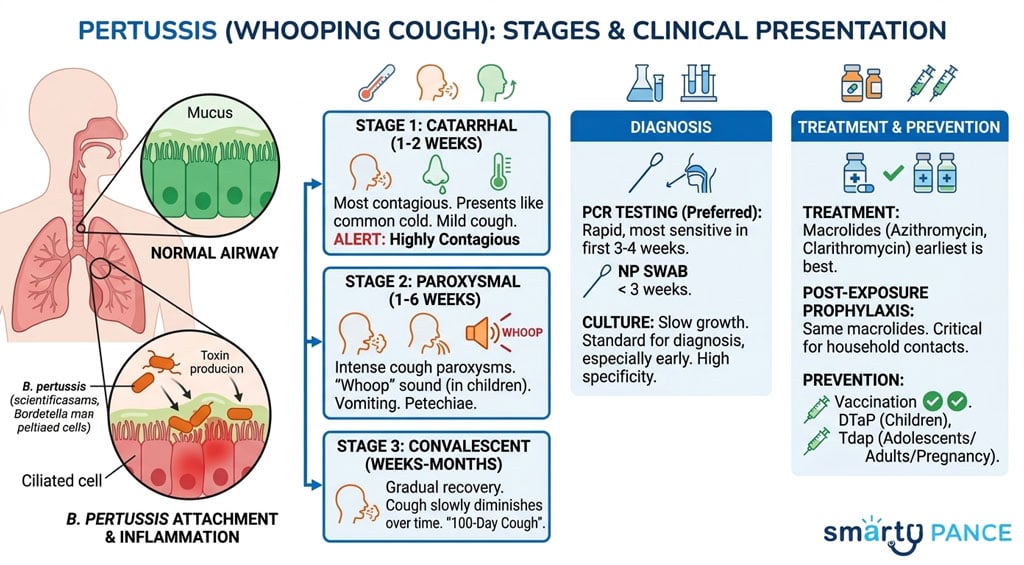 Whooping cough (pertussis) is a highly contagious respiratory tract infection marked by a severe hacking cough followed by a high-pitched intake of breath that sounds like a whoop. Whooping cough (pertussis) is a highly contagious respiratory tract infection marked by a severe hacking cough followed by a high-pitched intake of breath that sounds like a whoop.
Diagnosed by a nasopharyngeal swab of nasopharyngeal secretions – culture Tx: macrolide antibiotic - preferred: azithromycin or clarithromycin
|
||||||||||||||||||||||||||||||||||||
| Pneumonia (PEARLS) |
Presentation: Tachycardia, tachypnea, dyspnea, febrile, age 65+ Physical exam: Egophony, fremitus, rales Chest radiograph: Infiltrates and or consolidation Treatment: Community-Acquired
Hospital-Acquired (HAC): Vancomycin + Piperacillin/Tazobactam AIDs patients receive Bactrim prophylaxis against PJP pneumonia
CURB-65 Score for Pneumonia Severity
|
||||||||||||||||||||||||||||||||||||
| Respiratory syncytial virus infection (ReelDX) | Patient will present as → a 5-month-old infant with a three-day history of a mild respiratory tract infection with serous nasal discharge, fever of 38.5 C, and decreased appetite. Physical exam reveals a tachypneic infant with audible wheezing and a respiratory rate of 65. Nasal flaring, use of accessory muscles, subcostal and intercostal retractions are noted. Expiratory wheezes and cough are present. MC cause of lower respiratory tract infection in children worldwide – virtually all get it by age 3; the leading cause of pneumonia and bronchiolitis
Tx: Indications for hospitalization ⇒ tachypnea with feeding difficulties, visible retractions, oxygen desaturation < 95-96%
Vaccination (view current CDC guidelines)
Infants and young children
Prophylaxis: Palivizumab (Synagis) prophylaxis, FDA-approved for children at high risk for severe RSV disease
See Bronchiolitis |
||||||||||||||||||||||||||||||||||||
| Tuberculosis (ReelDx) | ReelDx Virtual Rounds (Tuberculosis)Patient will present as → 34-year-old female nurse presents with a worsening cough of six weeks’ duration together with weight loss, fatigue, night sweats, and fever. A recent HIV test was negative. A CT scan of the chest reveals a 3 cm lesion in the upper lobe of the left lung and calcification around the left lung hilus. A sputum smear was positive for acid-fast organisms. Tuberculosis (TB) is a disease caused by bacteria called Mycobacterium tuberculosis (acid-fast bacilli)
Screening with tuberculin skin test (TST) or interferon-gamma release assays IGRAs Mantoux Test Rules: The test is positive if induration
Diagnosis with sputum for AFB smears and Mycobacterium tuberculosis cultures – have to be 3 AFB negative
TX: If PPD/IGRA is POSITIVE, order a CXR
PPD positive or IGRA + CXR negative = latent TB ⇒ CDC recommends short-course, rifamycin-based, 3- or 4-month latent TB infection treatment regimens over 6- or 9-month isoniazid monotherapy
PPD positive or IGRA + CXR positive = active TB ⇒ Several treatment regimens are recommended in the United States for active TB disease. TB treatment can take 4, 6, or 9 months depending on the regimen.
All are hepatotoxic, so you need to get baseline labs
Monitor serum creatinine; take meds on an empty stomach since food can reduce absorption, watch for hepatotoxicity, be aware of drug interactions, especially with HIV meds  Upper cavitary lesion on CXR associated with Tb  A case of long-standing tubercular lymphadenitis with sinus |


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}