 Lecture
Lecture
Patient will present as → a 38-year-old African-American woman who visits the clinic complaining of persistent dry cough, shortness of breath, and mild chest pain for the past two months. She also notes occasional fevers and unexplained weight loss. You note erythema nodosum on her lower legs. Her chest X-ray reveals bilateral hilar lymphadenopathy and reticular opacities. Pulmonary function tests show a restrictive lung disease pattern. Laboratory findings include elevated serum angiotensin-converting enzyme (ACE) levels. A biopsy of the lymph nodes obtained during bronchoscopy demonstrates noncaseating granulomas, consistent with a diagnosis of sarcoidosis.

To watch this and all of Joe-Gilboy PA-C's video lessons, you must be a member. Members can log in here or join now.
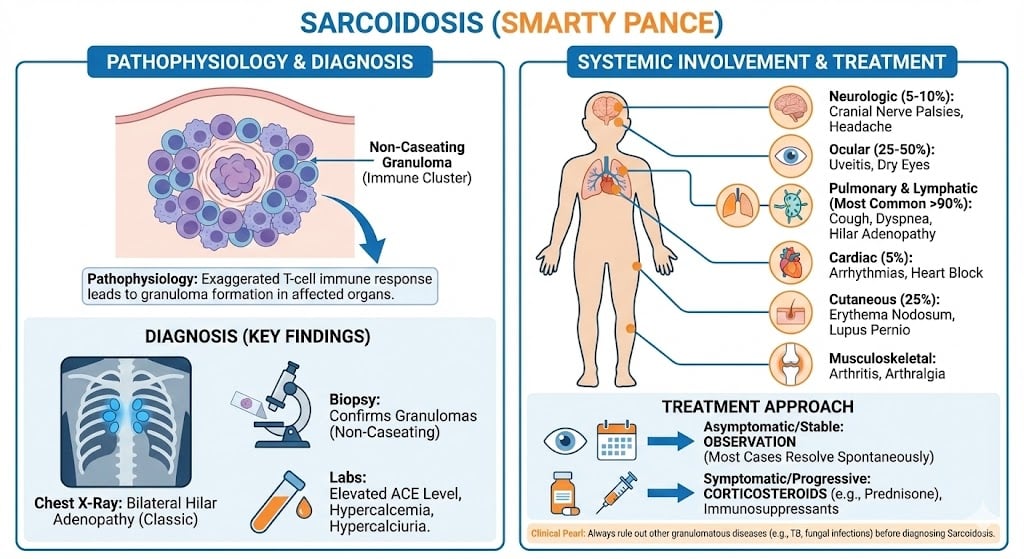
Sarcoidosis is a systemic granulomatous disease characterized by noncaseating (non-necrotizing) granulomas that can involve multiple organ systems
- The condition occurs mainly in persons aged 20 to 40 years and is most common in Northern Europeans and African Americans
- Sarcoidosis is caused by an abnormal T-cell–mediated immune response to an unknown environmental antigen in a genetically susceptible host, leading to the formation of non-caseating granulomas
- Certain individuals appear to have a genetic predisposition, and exposure to bacterial or viral antigens, organic dusts, or inorganic particles may act as the triggering stimulus
- Clinical presentation is variable. Fever, weight loss, arthralgias, and erythema nodosum (more common in Europeans) are typical early systemic features, while cough and dyspnea may be mild or even absent despite significant pulmonary involvement
- Bilateral hilar and mediastinal lymphadenopathy on chest radiograph is the hallmark finding and is present in up to 90% of cases
- Sarcoidosis causes elevated ACE and hypercalcemia because activated macrophages within granulomas produce ACE and convert inactive vitamin D into its active form, increasing intestinal calcium absorption

"If you see hilar lymphadenopathy, it is right to think Sarcoidosis, but not always. Here is a rough guide to approaching hilar adenopathy:
- Young female = Sarcoidosis
- Young kid with a fever, from Ohio, zookeeper = histoplasmosis
- Old guy in his 60's works on ceramics = Berylliosis"
Other manifestations include hepatic granulomas, granulomatous uveitis, polyarthritis, cardiac symptoms (including angina, CHF, and conduction abnormalities), cranial nerve palsies, and diabetes insipidus
Serum blood tests will show hypercalcemia and ACE levels 4 x normal
- ESR is often elevated
- Laboratory findings include leukopenia, hypercalcemia, hypercalciuria, and hypergammaglobulinemia (particularly in African American patients)
- Other abnormalities include elevated uric acid (not usually associated with gout), elevated alkaline phosphatase, elevated gamma-glutamyl transpeptidase, elevated levels of ACE, and pulmonary function tests showing restriction and impaired diffusing capacity
- Diagnosis can be made with a biopsy of peripheral lesions or fiber-optic bronchoscopy for central pulmonary lesions. Whole-body gallium scans can be used to show useful sites for biopsy and, in some cases, to follow disease progression
Serial pulmonary function tests are important for assessing disease progression and guiding treatment
"Hypercalcemia in sarcoidosis is due to the uncontrolled synthesis of 1,25-dihydroxyvitamin D3 by macrophages. 1,25-dihydroxyvitamin D3 leads to increased absorption of calcium in the intestine and to increased resorption of calcium in the bone."

Treatment for symptomatic patients consists of CORTICOSTEROIDS, methotrexate, and other immunosuppressive medications if steroid therapy is not helpful
- 90% of cases are responsive to corticosteroids and can be controlled with a modest maintenance dose
- ACE inhibitors for periodic hypertension
The prognosis depends on the severity of the disease. Spontaneous improvement is common; however, significant disability can occur with multiorgan involvement
- Pulmonary fibrosis is the leading cause of death.
 Osmosis Osmosis |
|
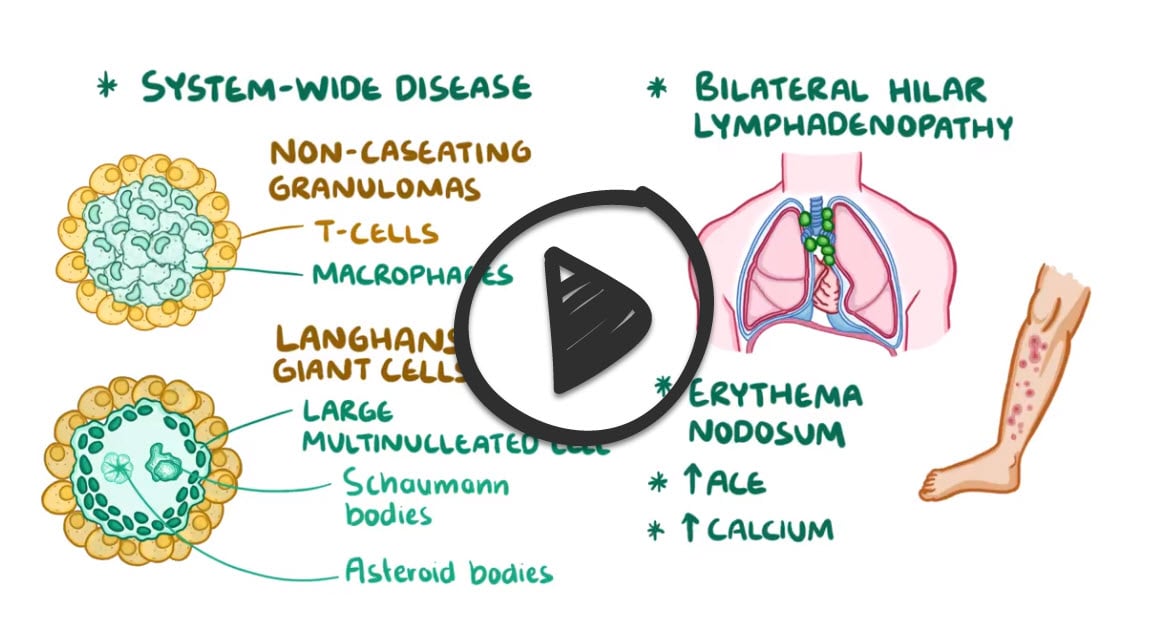 |
Sarcoidosis is an autoimmune disease characterized by noncaseating granulomas throughout the body. It is characterized by laboratory findings such as elevated ACE levels and asteroid bodies. Due to vitamin D activation, hypercalcemia is present. This disease is often asymptomatic and is diagnosed after finding bilateral hilar lymphadenopathy on a routine X-ray.
Play Video + QuizQuestion 1 |
Small cell carcinoma of the lung | |
Pulmonary tuberculosis | |
Sarcoidosis | |
Histoplasmosis | |
Asbestosis |
Question 2 |
Cryptogenic organizing pneumonia Hint: Cryptogenic organizing pneumonia is a type of diffuse interstitial lung disease that typically presents with cough, fever, dyspnea, and malaise. | |
Hypertensive encephalopathy Hint: Hypertensive encephalopathy manifests as headaches, vomiting, confusion, and neurological symptoms. The patient has none of these. | |
Cardiac sarcoidosis | |
Acute coronary syndrome Hint: Acute coronary syndrome is more likely to present with diaphoresis and crushing chest pain. | |
Pneumoconiosis Hint: Pneumoconiosis is a fancy word that means the accumulation of dust (e.g., coal, asbestos, etc.) within the lungs. This patient has absolutely nothing in his history that suggests this. |
|
List |
References: Merck Manual · UpToDate