
Patient with emphysema will present as → a 65-year-old male complaining of fatigue and shortness of breath with exertion. The patient reports minimal cough. On physical exam, you note a thin, barrel-chested man with decreased heart and breath sounds, pursed-lip breathing, end-expiratory wheezing, and scattered rhonchi. Chest X-ray reveals a flattened diaphragm, hyperinflation, and a small, thin-appearing heart. PFTs show a decreased FEV1/FVC ratio.
Emphysema is a form of COPD due to structural changes in the lung - air spaces are enlarged as a consequence of the destruction of alveolar septae
- Chronic bronchitis and emphysema almost always coexist
- Chronic bronchitis (clinical features - a productive cough) vs. Emphysema (structural changes - enlarged airspaces)
- Loss of elastin → Lungs more compliant (lungs expand, hold air)
- Alveolar air sacs permanently enlarge and lose elasticity → exhaling is difficult
Dyspnea and shortness of breath due to decreased gas exchange cause patients to exhale slowly through pursed lips to increase pressure in airways to keep airways from collapsing
- Individuals are able to oxygenate blood (pink), but they have to purse their lips to do so (puffers) = Pink Puffers!
- Alveoli are destroyed
- Barrel chest due to air trapping and hyperinflation of lungs
- CO2 retainers (due to loss of elasticity), the body must increase ventilation to blow off CO2
- Hyperinflation with bullae is a consistent finding in patients with emphysema
- CXR reveals loss of lung markings and hyperinflation, tall lung fields, flat diaphragms
- Normal hematocrit (HCT)
CXR reveals loss of lung markings, hyperinflation, increased anterior-posterior diameter
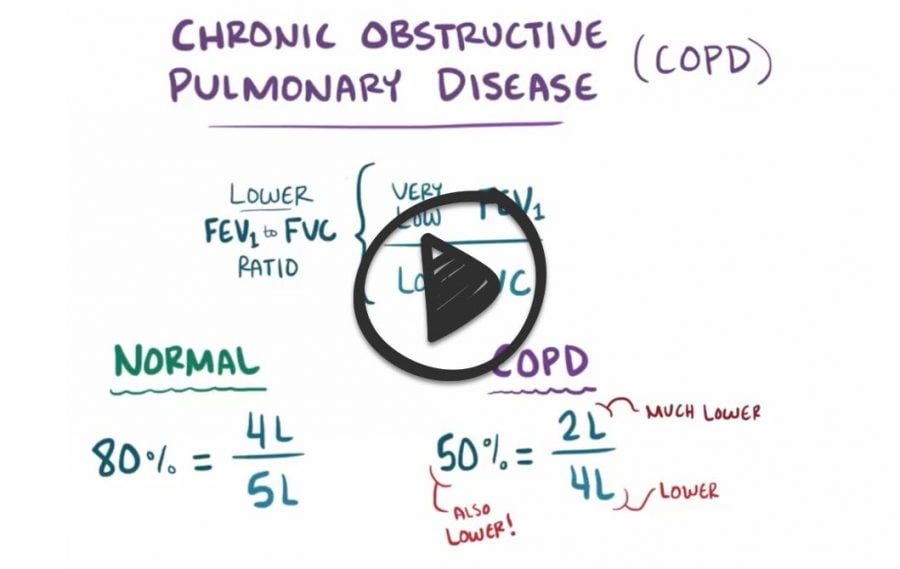
- PFTs show a decreased FEV1/FVC ratio + increased TLC (due to air trapping)

The most effective therapy for most patients with emphysema is smoking cessation
- Treatment depends on severity: a combination of short-acting (SABA) or long-acting (LABA) beta 2 agonist and short-acting (SAMA) or long-acting (LAMA) muscarinic agent (also known as an anticholinergic agent) +/- inhaled glucocorticoids
- Long-term oxygen therapy in all patients with COPD who have chronic hypoxemia defined as (SpO2) ≤ 88%
- Vaccination against both influenza and pneumococcal disease
- COPD exacerbations are managed with systemic glucocorticoids, antibiotics (tailored to the likelihood of specific pathogens), and antiviral therapy when influenza is suspected
 Osmosis Osmosis |
|
 |

Emphysema is a form of chronic obstructive lung disease characterized by the destruction of alveolar walls. There are two main forms of emphysema. Centriacinar emphysema is the most common form and associated with many years of smoking. Panacinar emphysema is less common and associated with individuals with an alpha-1 antitrypsin deficiency. Overall, emphysema is characterized by increased elastase activity, increased lung compliance, enlargement of air spaces, and decreased recoil of the lungs. Individuals with emphysema are commonly called pink puffers and have increased anteroposterior diameter of the chest, often referred to as a barrel chest. They also commonly exhale through pursed lips which help keep their airways open during exhalation.
Play Video + QuizQuestion 1 |
Home oxygen therapy Hint: Home oxygen therapy is indicated in COPD patients with an oxygen saturation < or equal to 88% or a pO2 < or equal to 55 mm Hg taken at rest breathing room air. | |
Maintenance oral steroids Hint: While oral steroids may be utilized in treatment of COPD, they are usually reserved for end stage disease due to the multiple systemic side effects of prolonged use. In addition only about 10% of patients show any increase in FEV1 and there use should be reserved for patients who show a 20% or greater improvement in FEV1. | |
Prophylactic antibiotic therapy Hint: Use of antibiotics should be reserved for treatment of acute exacerbations of COPD, acute bronchitis or documented bacterial infections, not prophylaxis. | |
Recommend influenza and pneumococcal vaccines |
Question 2 |
Interstitial inflammation and fibrosis Hint: Interstitial inflammation and fibrosis are seen with restrictive causes of lung disease, such as asbestosis. | |
Alveolar enlargement and loss of septa | |
Mucosal edema and inflammatory response Hint: Mucosal edema and inflammatory response are seen with asthma. | |
Excessive mucus secretion and chronic cough Hint: Excessive mucus secretion and chronic cough are characteristic of chronic bronchitis. |
Question 3 |
Increased tactile fremitus Hint: Physical examination findings in emphysema include a midline trachea, diffuse hyperresonant to percussion, and decreased tactile fremitus. | |
Dullness to percussion Hint: See A for explanation. | |
Distant heart sounds | |
Deviated trachea Hint: See A for explanation. |
Question 4 |
Broad-spectrum antibiotic | |
Admission to the hospital Hint: Admission is only warranted if the patient's respiratory status requires ventilatory assistance. This patient's blood gases are unremarkable for a patient with COPD and the patient is not in respiratory distress. | |
Oxygen at 6 L/min by nasal cannula Hint: Oxygen therapy should only be used for severe hypoxemia and should only be given at a low concentration, such as 2 L/min. Higher dose oxygen may stop the hypoxemic ventilatory drive. | |
Brief course of oral theophylline Hint: Oral theophylline is considered a secondary bronchodilator. The use of a metered-dose inhaler would be a preferable first-line treatment if this method of treatment were chosen. |
Question 5 |
Emphysema | |
Pulmonary fibrosis Hint: The PFTs from a person with pulmonary fibrosis would be consistent with a restrictive pattern. This patient has an obstructive pattern of lung disease. | |
Ventricular septal defect Hint: Ventricular septal defect will have a systolic murmur associated with it. | |
Congestive heart failure Hint: Congestive heart failure might explain some of the symptoms of this patient (increasing shortness of breath and DOE), he denies other common symptoms, such as orthopnea and peripheral edema. CHF should not result in changes in the PFTs. |
Question 6 |
Persistent asthma Hint: Lung function in asthma is evaluated by FEV1/FVC ratio with reduction noted with airflow obstruction. | |
Chronic obstructive pulmonary disease | |
Idiopathic fibrosing interstitial pneumonia Hint: Pulmonary function testing in idiopathic fibrosing interstitial pneumonia shows a loss of lung volume with normal to increased airflow rates in interstitial lung disease. | |
Sarcoidosis Hint: Restrictive changes with decreased lung volumes and diffusing capacity are common in sarcoidosis. |
|
List |
References: Merck Manual · UpToDate