NCCPA™ PANCE Eyes, Ears, Nose, and Throat Content Blueprint eye disorders ⇒ corneal disorders
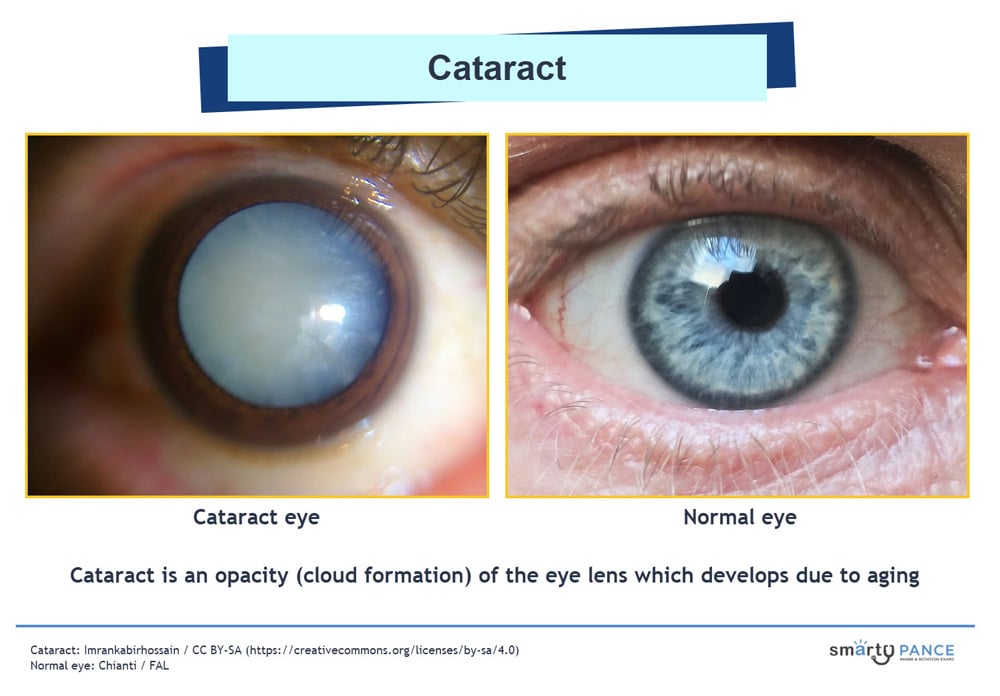
| Cataract | Patient presents as → a 78-year-old man who complains of slowly progressive vision loss over the last several years. He describes his vision as if he is looking through “dirty glass” and reports seeing a white halo around lights. On physical exam, there is a clouding of the lens and no red reflex. Blurred vision over months or years, halos around lights. Clouding of the Lens (versus clouding of cornea = glaucoma)
DX: is by fundoscopy "black on red background" ⇒ cataract appears dark against the red reflex on exam
Tx: Surgical removal is definitive
|
| Corneal ulcer | Patient will present as → a 34-year-old contact lens wearer with severe pain, redness, and photophobia. Eyes are injected with cloudy discharge unilaterally. A dense corneal infiltrate is visible with fluorescein staining. Contact lens wearers - caused by a deep infection in the cornea by bacteria, viruses, or fungi.
DX: Fluorescein stain is diagnostic
TX: Immediate referral - if an immediate referral is not possible, it is reasonable to start topical ophthalmic antibiotics without delay Corneal Ulcers vs. Keratitis The main difference between a corneal ulcer and keratitis is that a corneal ulcer is an open sore on the cornea, while keratitis is a general term for inflammation of the cornea. Not all cases of keratitis lead to corneal ulcers, but a corneal ulcer is always accompanied by keratitis!
 Corneal Ulcer as visualized with and without stain |
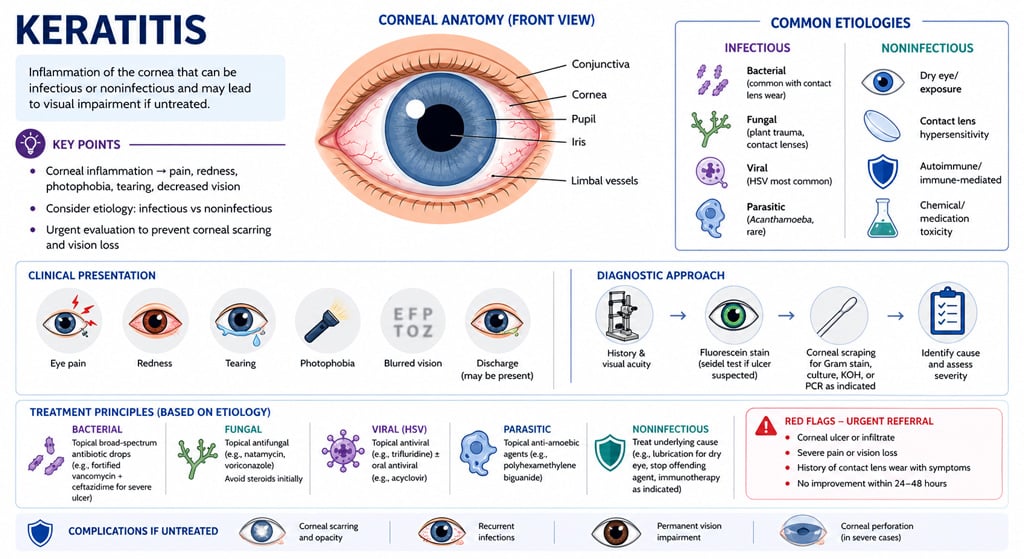
| Keratitis and infectious corneal disorders | Patient will present as → a 37-year-old female with intense, tearing pain in her right eye. She was recently placed on topical corticosteroids for suspected allergic conjunctivitis. On visual inspection, the conjunctiva appears red. A fluorescein stain of the eye exhibits a shallow ulcer with a dendritic appearance and irregular borders.
Keratitis is inflammation of the cornea that can lead to vision loss if not treated promptly, and may be infectious or non-infectious in origin.
TX: Depends on etiology:
Urgent ophthalmology referral is essential to prevent corneal scarring and vision loss |
| Pterygium (ReelDx) | ReelDx Virtual Rounds (Pterygium)Patient will present as → a 65-year-old male Hispanic farmworker who is brought to you by his concerned wife. She reports he has had this “thing” on his left eye for years and refuses to seek care. He denies pain or discharge from the affected eye. Physical exam reveals an elevated, superficial, fleshy, triangular-shaped fibrovascular mass in the inner corner/nasal side of the left eye. Elevated, superficial, fleshy, triangular-shaped “growing” fibrovascular mass (most common in the inner corner/nasal side of the eye).
DX: This is a clinical diagnosis TX: Observation: for small, asymptomatic pterygia not threatening the visual axis
.jpg) Superficial, fleshy, triangular-shaped “growing” fibrovascular mass (most common in the inner corner/nasal side of the eye) |

{kind=link}
{kind=link}
{kind=link}
{kind=link}