NCCPA™ PANCE Eyes, Ears, Nose, and Throat Content Blueprint eye disorders ⇒ lacrimal disorders
Lacrimal gland vs. lacrimal sac vs. lacrimal duct
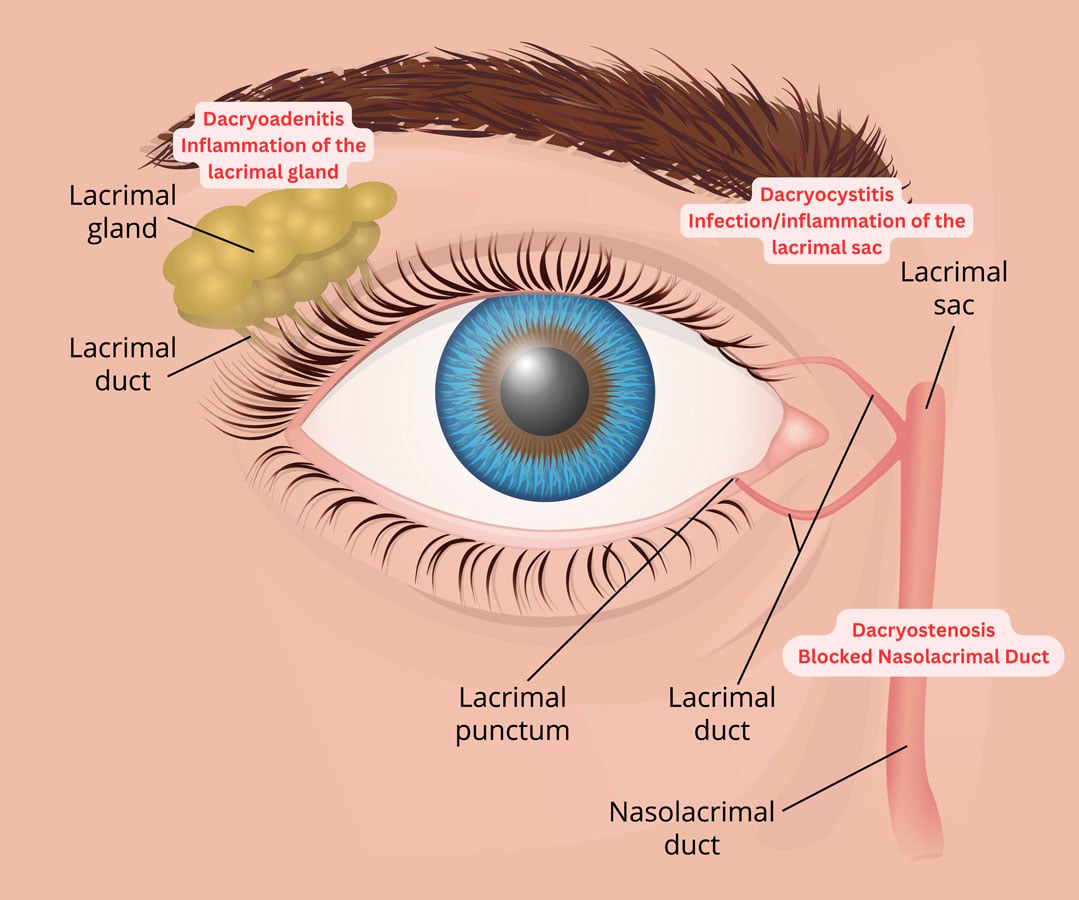
Image © by Adobe Stock (with edits by Smarty PANCE)
The lacrimal gland makes tears, while the lacrimal sac temporarily stores tears (made in the lacrimal gland), preventing them from constantly flooding the lacrimal ducts. The lacrimal duct, or the nasolacrimal duct, drains tears into the nasal cavity.
| Feature | Dacryostenosis | Dacryoadenitis | Dacryocystitis |
|---|---|---|---|
| Definition | Obstruction of the nasolacrimal duct. | Inflammation of the lacrimal gland. | Infection of the lacrimal sac. |
| Location | Medial canthus (tear duct). | Upper outer (lateral) eyelid. | Medial canthus (nasal side). |
| Cause | Congenital or acquired duct obstruction | Viral or bacterial infection; rarely autoimmune | Bacterial infection (e.g., Staphylococcus, Streptococcus) |
| Symptoms | Chronic tearing (epiphora), mild crusting, reflux of mucus when pressed. | "S-shaped" eyelid deformity, pain, and swelling in the outer lid. | Severe pain, redness, and swelling over the sac; purulent discharge. |
| Age Group | Most common in infants (congenital). | Young adults; often post-viral (Mumps/EBV). | Infants or older adults. |
| Treatment | Lacrimal sac massage (Crigler) + warm compresses; probing if persistent. | Cool compresses, NSAIDs (viral), or antibiotics (bacterial). | Systemic antibiotics (Augmentin); Do NOT probe during acute infection. |
| Dacryoadenitis and Dacryocystitis | Dacryoadenitis
Patient with dacryoadenitis will present as → a 32-year-old woman presents to the emergency department with a 2-day history of pain, redness, and swelling in the outer corner of her right eye. She denies any vision changes, discharge, or trauma. She has no significant past medical history and is not on any medications. On physical examination, you note localized erythema and swelling over the lateral aspect of her right upper eyelid. Her visual acuity is normal, and there is no proptosis. Dacryoadenitis is the inflammation of the lacrimal (tear-producing) gland, commonly caused by infection (bacterial or viral) or systemic inflammatory conditions (supratemporal)
DX: The diagnosis is based on clinical observation, but imaging (e.g., CT or MRI) can confirm lacrimal gland involvement and rule out abscess or neoplasm TX: Acute treatment involves:
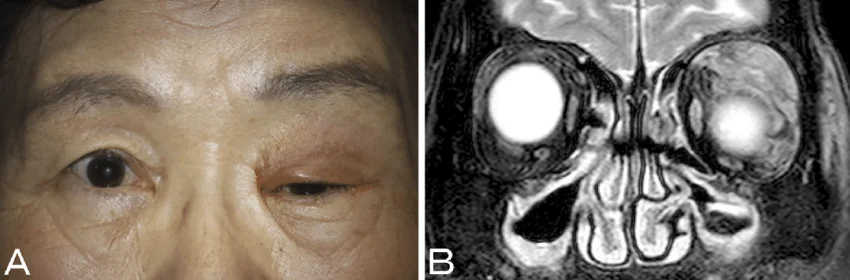 Dacryoadenitis presenting as an erythematous, swollen upper eyelid and ptosis. From "Dacryoadenitis with Ptosis and Diplopia as the Initial Presentation of Granulomatosis with Polyangiitis" by Makoto Hibino and Tetsuri Kondo via ResearchGate. Licensed under CC BY-NC-ND 4.0. Dacryocystitis Patient with dacryocystitis will present as → a 58-year-old woman presents to the emergency department with a 3-day history of increasing pain, redness, and swelling in the inner corner of her left eye. She also reports some purulent discharge from the same eye. She denies any vision changes or trauma. On physical examination, you note localized erythema, warmth, and swelling over the medial canthal area of her left eye. Her visual acuity is normal. Dacryocystitis is an infection or inflammation of the lacrimal sac, typically caused by obstruction of the nasolacrimal duct
DX:
TX:
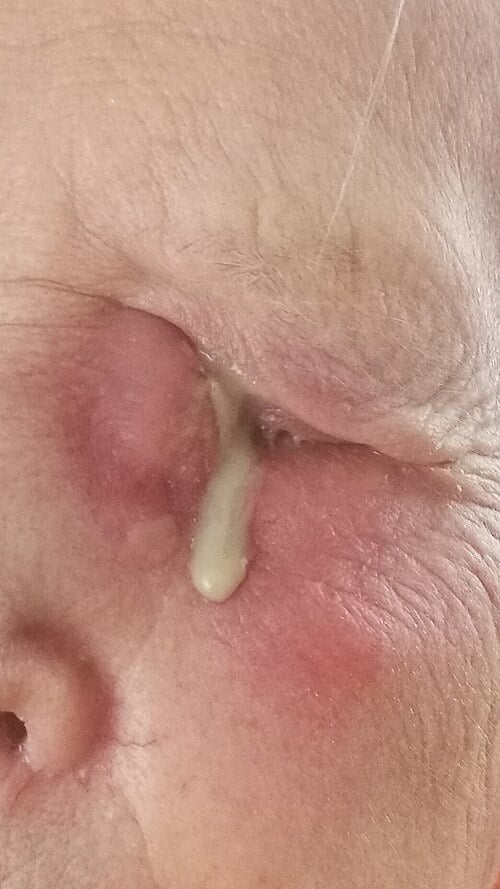 Dacryocystitis with swelling and inflammation over the lacrimal sac. Photo by Natanalyzator via Wikimedia Commons, CC BY-SA 4.0. 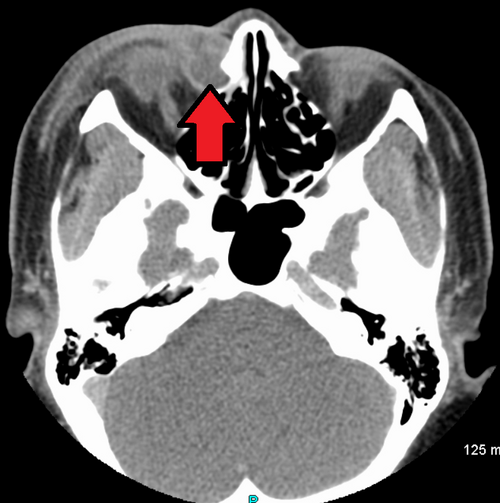 CT showing dacryocystitis with inflammation of the lacrimal sac adjacent to the medial orbit (arrow). Photo by James Heilman, MD via Wikimedia Commons, CC BY-SA 4.0.
|
| Dacryostenosis (Nasolacrimal Duct Obstruction) | Patient will present as → a 6-week-old female presents with persistent tearing and yellowish discharge from the left eye since birth. The parents deny redness or swelling. Physical exam shows tearing, mucopurulent discharge, and a normal conjunctiva. Gentle pressure over the lacrimal sac produces discharge. The patient is diagnosed with dacryostenosis. Management includes lacrimal sac massage and topical antibiotic ointment if needed. Symptoms are expected to resolve by 6 to 12 months; persistent cases may require referral for nasolacrimal duct probing. Dacryostenosis is a condition characterized by the obstruction of the nasolacrimal duct, leading to excessive tearing (epiphora).
DX: Diagnosis is clinical, based on symptoms and examination showing a blocked tear drainage system; additional tests like fluorescein dye disappearance test may help confirm obstruction TX: Initial management in infants involves lacrimal sac massage (Crigler maneuver) and monitoring, as many cases resolve spontaneously by 6-12 months
 Dacryostenosis (Blocked Tear Duct) |
| Keratoconjunctivitis sicca | The patient will present as → a 48-year-old woman who complains of chronic eye irritation, dryness, and a gritty sensation in both eyes. She notes that her symptoms worsen at night and after prolonged periods of reading or screen time. She reports mild discomfort with bright lights and occasional blurred vision. Her medical history includes rheumatoid arthritis. On examination, her eyes appear slightly reddened with decreased tear meniscus, and she blinks frequently. Given her symptoms and history of autoimmune disease, keratoconjunctivitis sicca (dry eye syndrome) is suspected. A Schirmer’s test reveals tear production of less than 5 mm in 5 minutes, confirming significantly reduced tear production. The patient is advised to use artificial tears frequently throughout the day and is prescribed an ophthalmic lubricating ointment for nighttime use. A follow-up visit is scheduled to monitor her response to therapy. Keratoconjunctivitis sicca, or dry eye syndrome, is characterized by chronic cornea and conjunctiva dryness due to insufficient tear production or increased tear evaporation
DX: Relies on clinical symptoms and tests like Schirmer's Test, Tear breakup test (TBUT), and fluorescein staining TX: Include artificial tears, anti-inflammatory eye drops, environmental modifications, and punctal plugs to relieve symptoms and prevent complications like corneal ulcers or vision impairment  Schirmer's test demonstrating the placement of the strip in the lower eyelid pouch. Created by Jmarchn via Wikimedia Commons. Licensed under CC BY-SA 3.0. |
{kind=link}