NCCPA™ PANCE EENT Content Blueprint ⇒ ear disorders
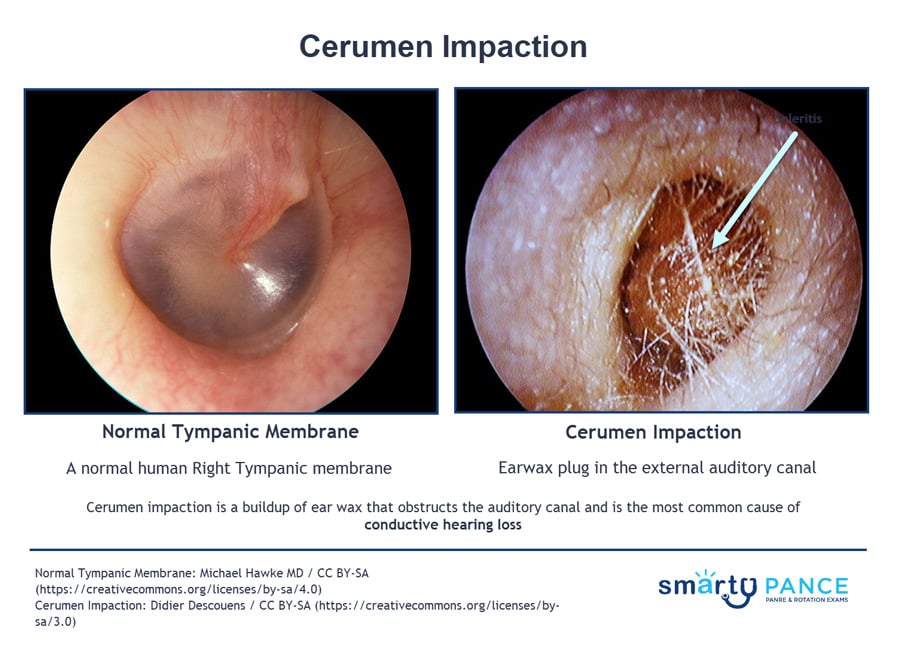
| Cerumen Impaction | Patient will present as → a 25-year-old patient presents with unilateral hearing loss. Weber reveals lateralization to the right ear. Rinne test reveals the following: RIGHT: bone conduction = 10 seconds, air conduction = 5 seconds; LEFT: bone conduction = 5 seconds, air conduction = 10 seconds. Cerumen impaction—buildup obstructs the auditory canal and is the most common cause of conductive hearing loss
DX: Diagnosis is clinical by otoscopy TX: Irrigation after several days of softening with carbamide peroxide (Debrox) or triethanolamine (Cerumenex)
|
| Otitis externa | Patient will present as → a 4-year-old girl who is brought to the clinic by her mother who states that the child has been complaining of progressively worsening ear pain and itchiness over the past week. Examination reveals left tragal tenderness and an edematous and closed canal. Weber lateralizes to the left. Bacterial otitis externa "swimmer's ear"
DX: Diagnosis is clinical by otoscopy TX:
DX: Diagnosis is clinical by otoscopy TX:
 Erythema, edema, and purulent drainage due to otitis externa |
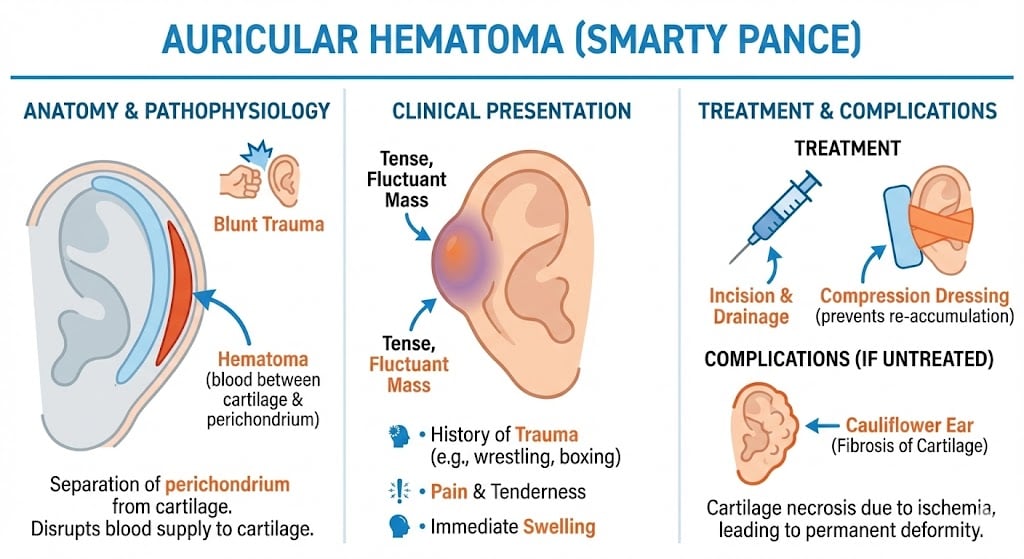
| External Ear Trauma | Patient will present as → a 17-year-old on the high school varsity wrestling team who was injured during a match. On physical exam, you note a fluctuant, tender edematous lesion of the anterior-superior outer portion of the right pinna Trauma to the external ear may result in hematoma, laceration, avulsion, or fracture Subperichondrial hematoma (cauliflower ear)
Lacerations: Lacerations can be partial, or it may go all the way through the ear (complete) Avulsions: The ear may be torn away from the head (avulsion). An ear may be partially or completely torn Fractures: A forceful blow to the jaw may break (fracture) the bones around the ear canal and distort the canal’s shape, often narrowing it DX: The diagnosis of auricular hematoma is made by the characteristic clinical appearance in patients with a history of blunt trauma to the auricle
TX:
 Acute hematoma of the right ear  Cauliflower ear |
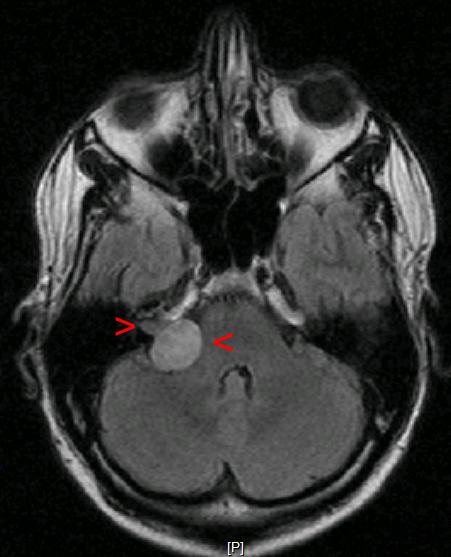
| Acoustic neuroma | Patient will present as → a 42-year-old male with a history of neurofibromatosis type II, complaining of nausea, vomiting, headache, continuous disequilibrium, and a slowly progressive unilateral hearing loss in his right ear. On physical exam, the patient has decreased sensation to touch on the right side of his face. An MRI is performed, with results seen here. Benign tumor of the Schwann cells (the cells which produce myelin sheath) – most commonly affects the vestibular division of the 8'th cranial nerve.
DX: Definitive diagnosis is by MRI (Gold standard)
TX: Surgery or stereotactic radiation therapy
|
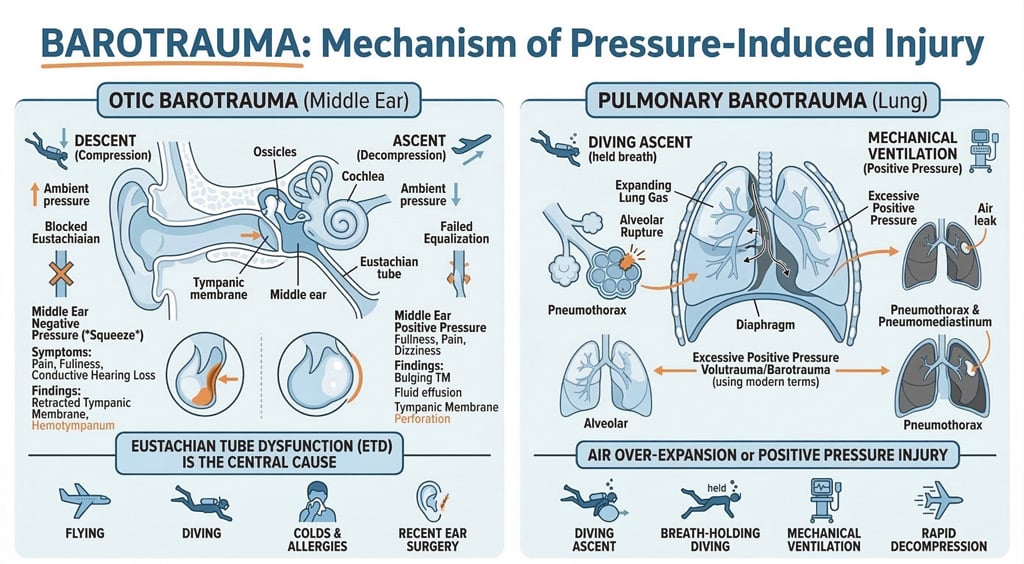
| Barotrauma | Patient will present as → a 17-year-old male who returned from a senior class trip to Mexico. While there, they decided to take scuba classes. After 3 days of shallow diving, they attempted their first 100-foot dive. After 5 minutes on their second dive, his equipment failed. He quickly shared the working breathing equipment of his friend, and they rose rapidly to the surface in a panic for air. The patient noticed immediate pain in his right ear, which resolved somewhat when he forcefully yawned and heard a “pop.” Since then, he reports dizziness and hearing loss in the affected ear. Barotrauma presents with ear pain and hearing loss that persists past the inciting event, associated with pressure changes
DX: clinical diagnosis, but sometimes requires imaging tests
TX: Supportive (anti-inflammatories), then consider prophylaxis
|
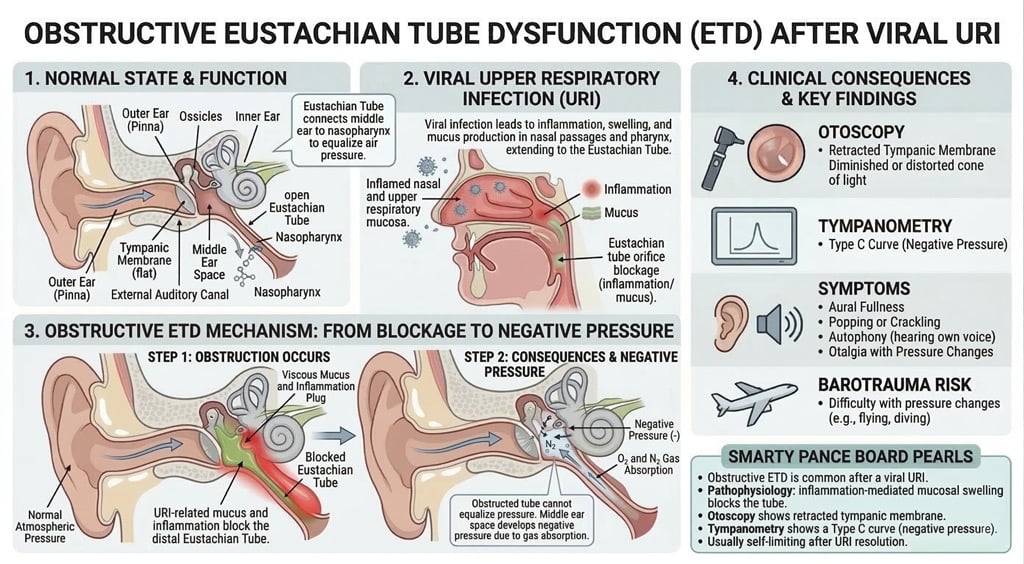
| Dysfunction of the eustachian tube | Patient will present as → a 9-year-old female with right otalgia and a nonproductive cough for one day. The patient complains of constant popping in her ears and fluctuating conductive hearing loss with tinnitus. The patient has no significant past medical history, her immunizations are up to date, and both of her parents are non-smokers. On otoscopic examination, the tympanic membranes are grey with normal landmarks, including visualization of the middle ear ossicles. There is no evidence of bulging pus or exudate suggestive of an acute inflammatory process. Ear fullness, popping of ears, underwater feeling, intermittent sharp ear pain, fluctuating conductive hearing loss, tinnitus.
DX: An excellent otoscopic exam is the key to making this diagnosis – otoscopic findings are usually normal. May see fluid behind TM if acute serous otitis media
TX: Often, no treatment is necessary
|
| Labyrinthitis | Patient will present as → 57 yo female with a six-day history of severe continuous dizziness associated with ataxia and right-sided hearing loss. She had an upper respiratory tract infection one week ago. Acute onset, continuous vertigo + hearing loss, tinnitus of several days to a week
DX: Labyrinthitis is a clinical diagnosis in the absence of neurologic deficits
TX:
Labyrinthitis is associated with CONTINUOUS vertigo along with hearing loss +/- tinnitus and is usually associated with an upper respiratory infection. This differentiates it from Meniere’s syndrome, which is EPISODIC and not typically associated with a viral infection. The features of acute labyrinthitis are similar to those of vestibular neuronitis, except labyrinthitis includes significant sensorineural hearing loss, which is NOT present in vestibular neuronitis. |
| Vertigo | ReelDx Virtual Rounds (Vertigo )Patient will present as → a 29-year-old male with intense nausea and vomiting that began yesterday. He states that he ran a 5K race in the morning and felt well while resting afterward. However, when he arose, he experienced two episodes of emesis accompanied by a sensation that the world was spinning around him. This lasted about one minute and subsided. He denies tinnitus or hearing changes but feels imbalanced. He has a PMH of migraines, but he typically does not have nausea or vomiting with migraine episodes. His temperature is 98.7°F, blood pressure is 132/82 mmHg, pulse is 75/min, and respirations are 13/min. The cardiopulmonary exam is unremarkable. Cranial nerves are intact, and gross motor function and sensation are within normal limits. When the patient’s head is turned to the right side and lowered quickly to the supine position, he claims that he feels “dizzy and nauseous.” Nystagmus is noted in both eyes. The sensation of movement (spinning, tumbling, or falling) in the absence of actual movement or an overresponse to movement
Central vertigo
Peripheral vertigo (inner ear)
DX:
Treatment:
|
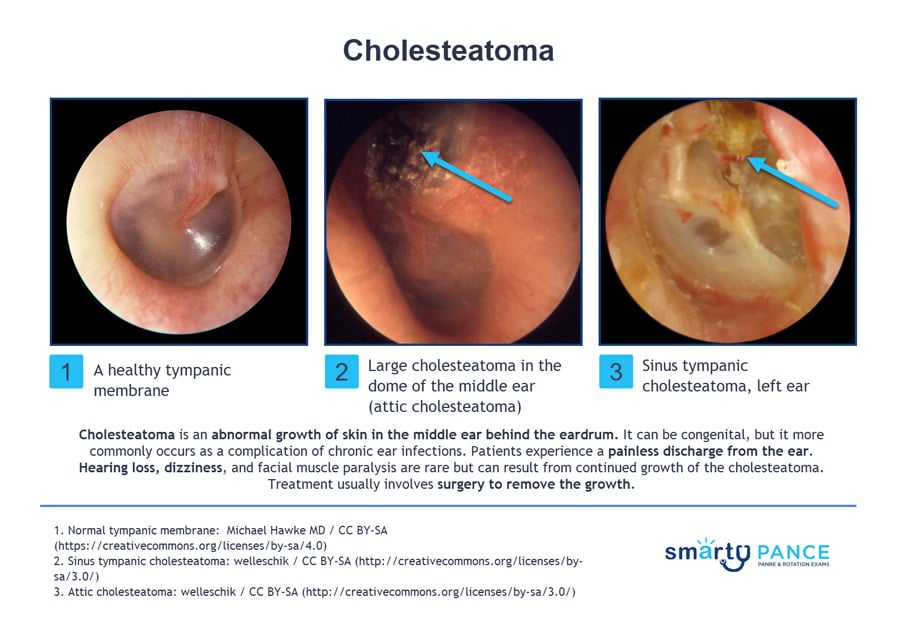
| Cholesteatoma | Patient will present as → a 43-year-old male with a “lifelong” history of chronic ear infections and episodic purulent drainage from his right ear canal. The patient is currently without symptoms. Examination of the ear shows a clear external canal, but the tympanic membrane is retracted, and there is a pocket of white material and an opacity of the pars flaccida. The Weber test lateralizes to the right, and Rinne shows air conduction > bone conduction on the left and bone conduction > air conduction on the right. Preparations are made to undergo a non-contrast computed tomography (CT) scan of the temporal bone. Cholesteatoma presents with painless otorrhea, brown/yellow discharge with a strong odor
DX: Diagnosis can be made with otoscopic visualization of granulation tissue
TX: Surgical removal
|
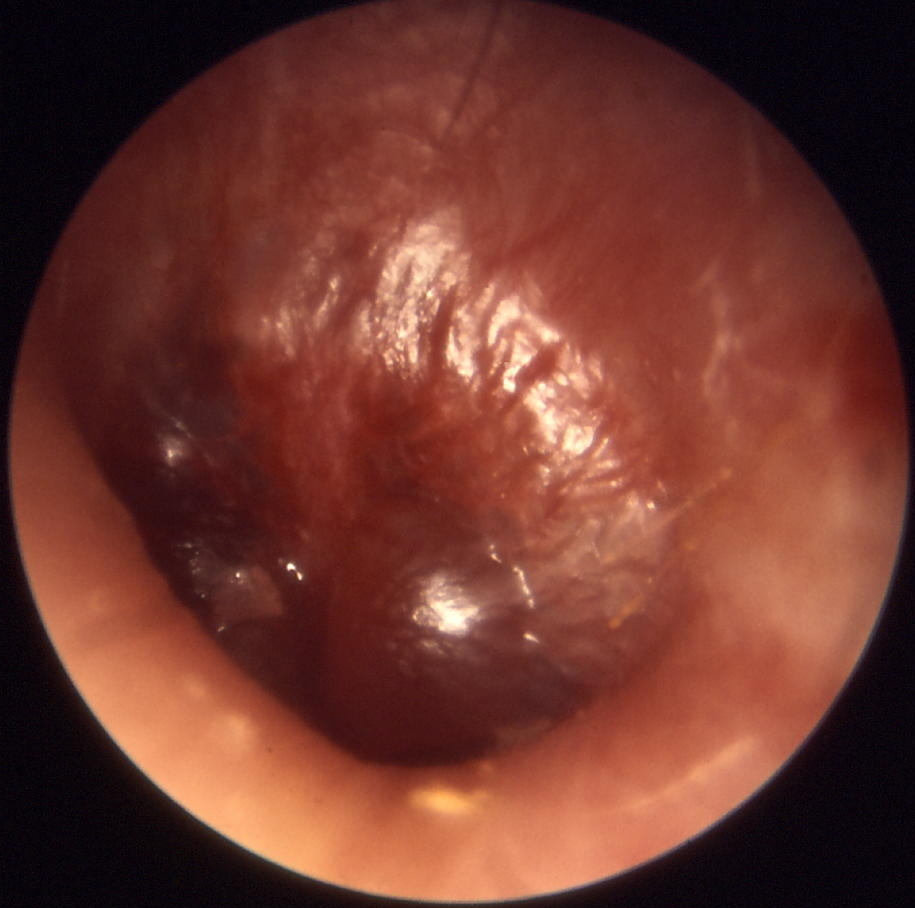
| Otitis media | ReelDx Virtual Rounds (Otitis media)Patient will present as → a 3-year-old previously healthy male is brought to your office by her mother. The mother reports the child has been crying and pulling at her right ear over the past 2 days and reports the patient has been febrile the past 24 hours. The patient’s past medical history is unremarkable, although the mother reports the patient had a “common cold” a week ago, which resolved without intervention. His temperature is 101.6 F, blood pressure is 100/70 mmHg, pulse is 120/min, and respirations are 22/min. The otoscopic exam is seen here. The clinical diagnosis of AOM requires 1) bulging of the tympanic membrane or 2) other signs of acute inflammation (eg, marked erythema of the tympanic membrane, fever, ear pain) and middle ear effusion
DX: Otoscopic examination may reveal bulging, loss of landmarks, redness, injection of TM, and pus.
TX: First-line amoxicillin, second-line augmentin, macrolides if penicillin-allergic
 Bulging, loss of landmarks, redness, and injection of TM, and pus |
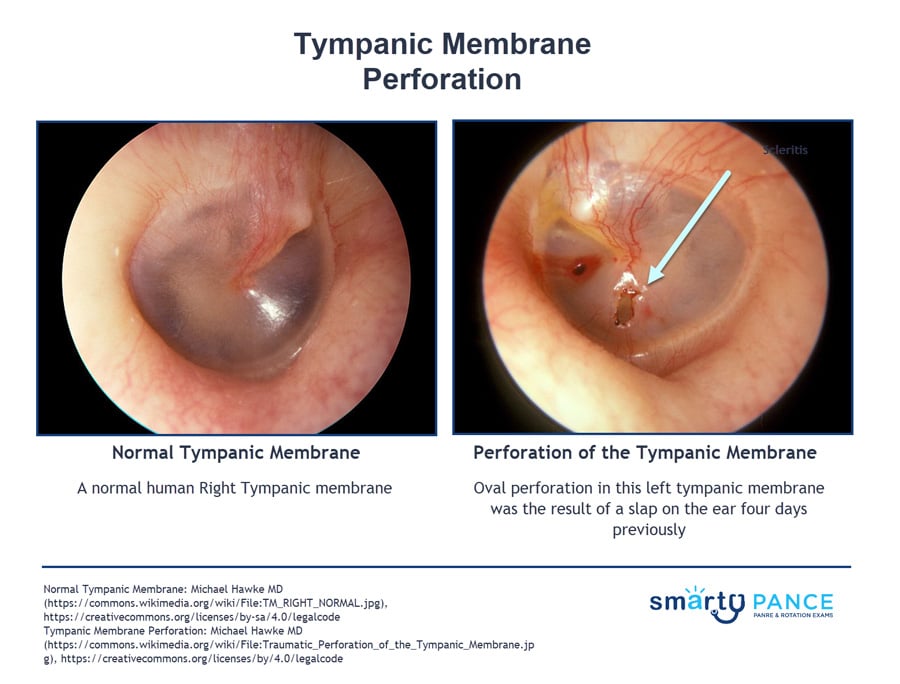
| Tympanic membrane perforation | ReelDx Virtual Rounds (Tympanic membrane perforation)Patient will present as → a 9-month-old female with nasal congestion and cough is brought to your clinic by her mother, who reports that the child is very fussy, has been tugging at her right ear, and refuses to eat. On physical exam, you note copious green/yellow nasal discharge and right-sided otorrhea. An otoscopic exam reveals a significant amount of clear/white discharge obstructing your view. With careful examination, you are able to observe a ruptured right tympanic membrane. Tympanic membrane perforation presents with pain, otorrhea, and hearing loss/reduction Diagnosis is based on otoscopy TX: Most heal spontaneously, keep clean and dry, treat with antibiotics
|
| Hearing impairment | Patient will present as → a 72-year-old male with a progressively worsening hearing loss. He states that his trouble with hearing began approximately 7-8 years ago. He is able to hear when someone is speaking to him; however, he has difficulty understanding what is being said, especially when there is background noise. In addition to his current symptoms, he reports a steady ringing in both ears and at times experiences dizziness. Medical history is significant for three prior episodes of acute otitis media. Family history is notable for his father being diagnosed with cholesteatoma. His temperature is 98.6°F (37°C), blood pressure is 138/88 mmHg, pulse is 14/min, and respirations are 13/min. On physical exam, when a tuning fork is placed in the middle of the patient’s forehead, the sound is appreciated equally on both ears. When a tuning fork is placed by the external auditory canal, and subsequently on the mastoid process, air conduction is greater than bone conduction. (presbycusis) Hearing loss can be classified as conductive, sensorineural, or both (mixed loss) Rinne and Weber Tests Conductive loss
Sensorineural loss
Sensorineural hearing loss
Conductive hearing loss
TX: Treat the underlying cause, hearing aids, surgery, cochlear implants |
| Mastoiditis | ReelDx Virtual Rounds (Mastoiditis )Patient will present as → a 10-year-old boy with otalgia, worsening over the last 5 days and associated with nasal congestion. The patient is afebrile with a temperature of 98 ° F. Examination reveals edema of the external auditory canal, producing an anterior and inferior displacement of the auricle with percussion tenderness posteriorly. A complication of acute otitis media. Fever, otalgia, pain & erythema posterior to the ear, and forward displacement of the external ear
DX: Clinical; CT scan temporal bone with contrast for complicated/toxic appearing TX: IV antibiotics (ceftriaxone), drainage of middle ear fluid
|
| Meniere disease | Patient will present as → 41-year-old female with intermittent episodes of vertigo, tinnitus, nausea, and hearing loss over the past week. Ménière syndrome is a disorder of the endolymphatic compartment with the classic triad of episodic vertigo, unilateral low-frequency sensorineural hearing loss, and tinnitus.  "Meniere's disease is associated with EPISODIC vertigo and NOT associated with viral infections. This differentiates it from Labyrinthitis, which is associated with CONTINUOUS vertigo along with hearing loss +/- tinnitus and is usually associated with an upper respiratory infection." DX: Although audiometric testing is a required part of the diagnostic evaluation, there is no specific diagnostic test for MD
A clinical diagnosis of MD is made based on the following criteria:
TX: Low salt diet, diuretics (HCTZ + triamterene) to reduce aural pressure |
| Tinnitus | Patient will present as → a 70-year-old female who states that her children and grandchildren have asked her to seek medical attention as she seems to be losing her hearing. She also describes an occasional ringing, buzzing, and hissing sound. She is in generally good health, and her only medications are a multivitamin along with calcium and vitamin D. You examine her ears and find the external auditory canals to be free of cerumen and the tympanic membranes to be normal in appearance. A perceived sensation of sound in the absence of an external acoustic stimulus is often described as ringing, hissing, buzzing, or whooshing.
DX: All patients with significant tinnitus should be referred for comprehensive audiologic evaluation to determine the presence, degree, and type of hearing loss.
TX: No pharmacologic agent has been shown to cure or consistently alleviate tinnitus
|
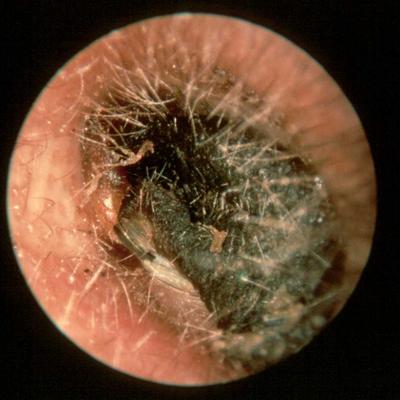
| Foreign body in ear (ReelDx) | ReelDx Virtual Rounds (Foreign body in ear)A foreign body in the ear is any object that gets stuck in the ear canal. This can include anything from small objects like beads and toys, to insects and food particles.
DX: On exam, the provider should visually inspect the ear canal with an otoscope. This may reveal swelling, abrasions, and the foreign body itself
TX: Removal should be attempted under direct visualization using warm irrigation with a syringe or instruments like an alligator forceps or a right-angle hook
|







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}