Patient will present as → a 42-year-old female presents to the clinic with complaints of a deep, aching pain in her right eye for the past week. She reports that the pain worsens with eye movement and has been severe enough to disrupt her sleep. She also notes redness and blurred vision in the affected eye but denies discharge or itching. Her medical history includes rheumatoid arthritis, diagnosed five years ago. On examination, the right eye shows diffuse redness involving the sclera and episclera with tenderness on palpation. Vision is mildly reduced in the affected eye. There is no evidence of discharge, corneal involvement, or proptosis. A slit-lamp examination reveals inflammation of the sclera without thinning or necrosis, consistent with diffuse anterior scleritis. Initial management includes oral NSAIDs, such as indomethacin, to reduce inflammation and relieve pain. The patient is referred to a rheumatologist for further evaluation and consideration of immunosuppressive therapy, such as methotrexate, if NSAIDs are insufficient. Close follow-up with an ophthalmologist is arranged to monitor response to treatment and evaluate for complications, such as scleral thinning or posterior scleritis.
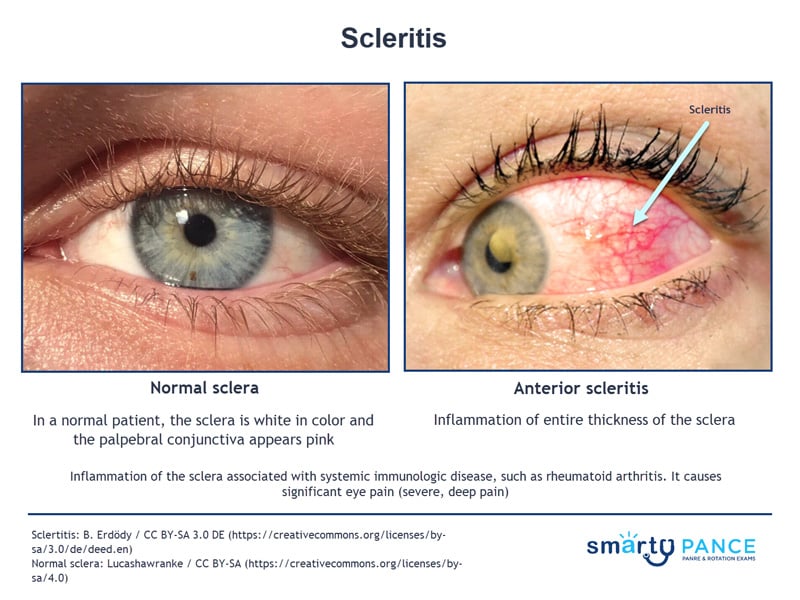
Inflammation of the sclera (the white outer coating of the eye) associated with systemic immunologic disease, such as rheumatoid arthritis
{kind=link}
- It causes significant eye pain (severe, deep pain), redness, photophobia, and reduced vision; pain often worsens with eye movement
- Types:
- Diffuse anterior scleritis (most common, least severe)
- Nodular anterior scleritis (localized nodules)
- Necrotizing scleritis (severe, may lead to scleral thinning and perforation)
- Posterior scleritis (rare, affects deeper scleral layers and adjacent structures)
On examination, there is ocular redness and pain on palpation of the eyeball. It can cause visual impairment
- Labs should include screening for systemic immunologic diseases, such as ANCAs, ANA, CRP, ESR, Lyme, RA, ACE, RPR, etc.
Refer the patient for prompt evaluation by an ophthalmologist
- NSAIDs (e.g., indomethacin) are effective for mild cases like diffuse or nodular anterior scleritis
- Glucocorticoids (e.g., prednisone 1 mg/kg/day) for severe cases or those unresponsive to NSAIDs
- Immunosuppressive agents (e.g., methotrexate, mycophenolate mofetil, or cyclophosphamide) for necrotizing scleritis or systemic disease involvement
- Biologic therapies (e.g., rituximab or TNF-alpha inhibitors) for refractory or severe cases
- Referral to an ophthalmologist + rheumatologist is essential for proper management and to address underlying systemic conditions
Question 1 |
Prescribe oral prednisone 1 mg/kg/day for one month | |
Prescribe topical prednisolone acetate 1% four times per day for one week Hint: Topical steroids can be used as the first-line agent in addition to oral NSAID treatment. | |
Discontinue ibuprofen Hint: The patient has not responded to first-line treatment but requires additional treatment to manage inflammation. | |
Prescribe topical artificial tears four times per day Hint: Artificial tears do not manage inflammation. They may provide some relief to any ocular surface dryness present. |
References: Merck Manual · UpToDate