 Osmosis
Osmosis

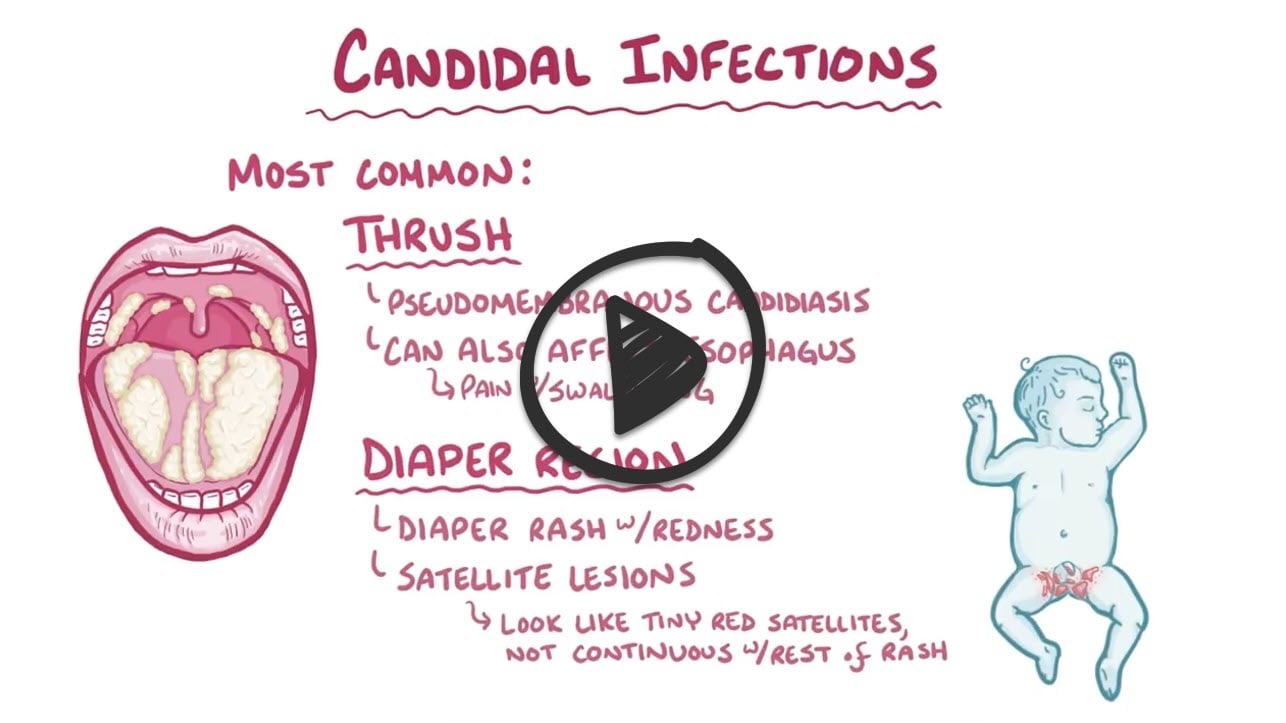
3-week-old with a black plaque on tongue and diaper rash
Patient will present as → a 3-week-old infant with decreased appetite and a rash in her mouth. On physical exam, you note white plaques on her tongue that scrape off with a tongue depressor and bleed slightly. Potassium hydroxide (KOH) preparation of the scrapings demonstrates budding yeasts with hyphae.
Alternative presentation → a 33-year-old HIV-positive female presents with her second episode of oral thrush in the past 2 months. Her current CD4 count is 75.
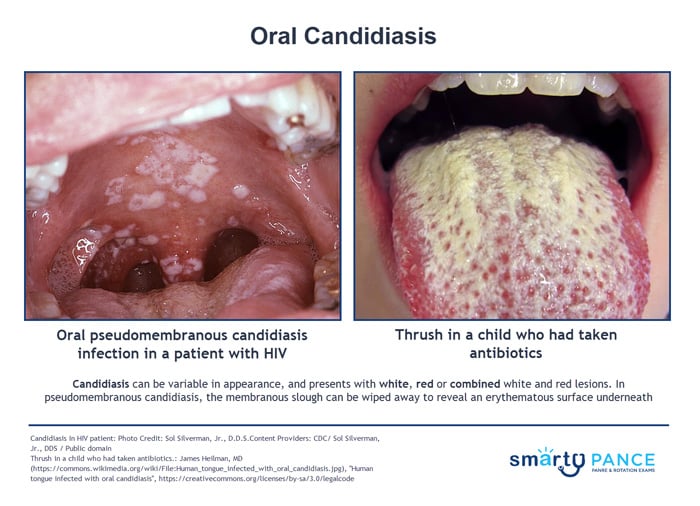
Oral candidiasis is a fungal infection of the mouth, often called 'thrush' because its white spots resemble the breast of a bird with the same name
{kind=link}
- Although Candida is present in 50% of the normal flora of healthy mouths, it causes infection (candidiasis) when increased numbers of yeast cells invade the mucosa
- Oropharyngeal candidiasis causes white plaques on oral mucous membranes that may bleed when scraped, but CAN be scraped off! (unlike oral leukoplakia, which does not scrape off)
- Remember, oral CANdidiasis = CAN scrape off
- If a patient has recurrent candidiasis look for underlying disorder => immunocompromised, long-term inhaled steroid use
Scrapes off with a tongue depressor, and it may bleed. (unlike oral leukoplakia, which does not scrape off)
- Potassium Hydroxide (KOH) prep for diagnosis: budding yeast/hyphae
- Confirmed with culture or tissue biopsy
Treatment is with antifungals, which are available in several forms (i.e., ketoconazole or fluconazole orally, clotrimazole troches, nystatin liquid rinses)
- Clotrimazole (Mycelex): oral 10-mg troche; 20 minutes 5 times daily for 7 to 14 days
- Nystatin oral suspension: 100,000 U/mL swish and swallow 400,000 to 600,000 U 4 times per day
- Treat infants with nystatin oral suspension 100,000 units to each cheek four times daily
- Nystatin pastilles: 200,000 U each, QID daily for 7 to 14 days
Question 1 |
A 72-year-old man with a history of poorly controlled diabetes presents to his primary care provider with a one-week history of white patches on his tongue and the inside of his cheeks. He also complains of a burning sensation in his mouth. Which of the following factors in this patient's history likely played the most significant role in the development of his current condition?
Smoking Hint: While smoking can be a risk factor for oral lesions and some infections, it isn't the primary or most direct contributor to oral candidiasis. | |
Recent antibiotic use Hint: Antibiotics can disrupt normal flora, but the risk relates to broad-spectrum coverage, not a primary driver of oral candidiasis in comparison to diabetes. | |
Poorly controlled diabetes | |
Use of inhaled corticosteroids Hint: This increases the risk of localized oral candidiasis due to medication remaining in the mouth, but the patient's uncontrolled diabetes would still be the major factor. | |
Vitamin B deficiency Hint: Vitamin B Deficiencies can have oral mucosal manifestations, but the presence of thrush and the risk factor of uncontrolled diabetes strongly outweighs this less direct connection. |
Question 2 |
Blood culture Hint: Does not identify organisms in the oral cavity. | |
Salivary pH Hint: Not helpful in diagnosis. | |
Oral glucose tolerance test Hint: Used to evaluate diabetes, not oral infections. | |
Potassium hydroxide preparation | |
Monospot testing Hint: Evaluates for EBV infection rather than fungal infection. |
Question 3 |
A 3-week-old otherwise healthy infant is brought to the pediatrician's office due to white plaques on the tongue and inner cheeks. The infant appears uncomfortable when nursing. The mother is breastfeeding and has no reported health concerns. Which of the following is the most appropriate first-line treatment for this infant?
Oral fluconazole Hint: Oral fluconazole is a systemic antifungal and generally not used as first-line treatment for mild oral candidiasis in infants due to potential side effects. | |
Clotrimazole oral troches Hint: Clotrimazole troches are not suitable for young infants due to choking risk. | |
Miconazole buccal tablets Hint: Similar to clotrimazole troches, they present a choking hazard for infants. | |
Systemic antibiotics Hint: Not effective against fungal infections and can exacerbate oral candidiasis by disrupting normal oral flora. | |
Nystatin oral suspension |
|
List |
References: Merck Manual · UpToDate