PANCE Inflammatory Disorders: Iritis (Anterior Uveitis), Scleritis, and Uveitis
| Iritis (Anterior Uveitis) | Scleritis | Uveitis |
 |
 |
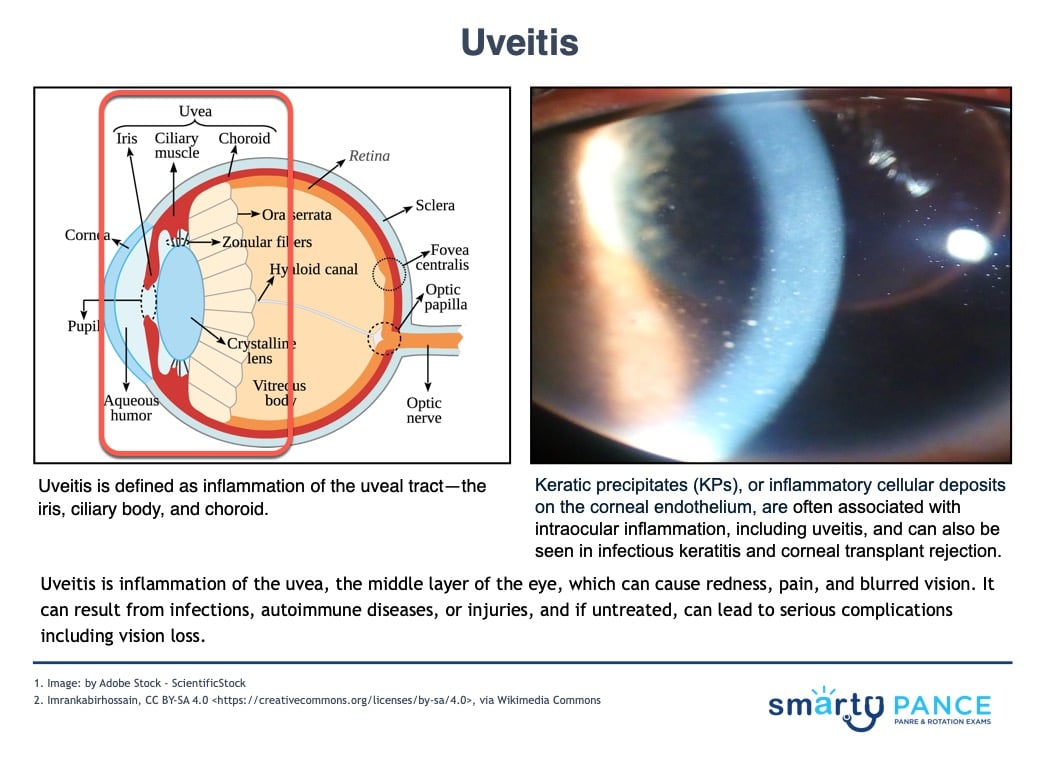 |
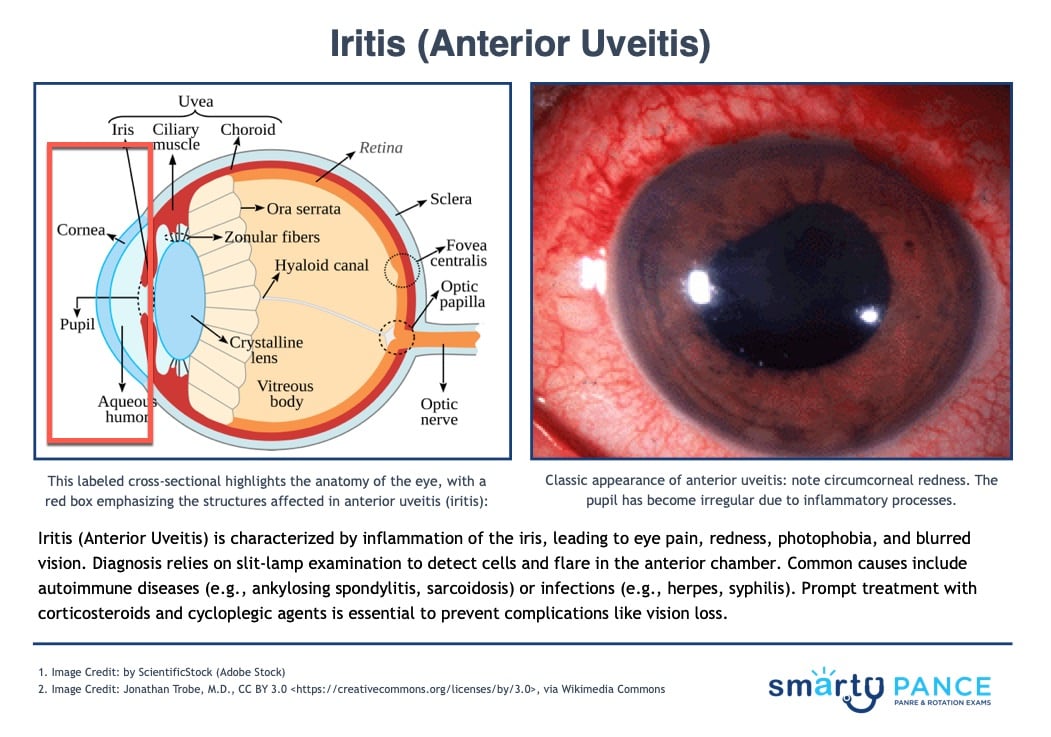
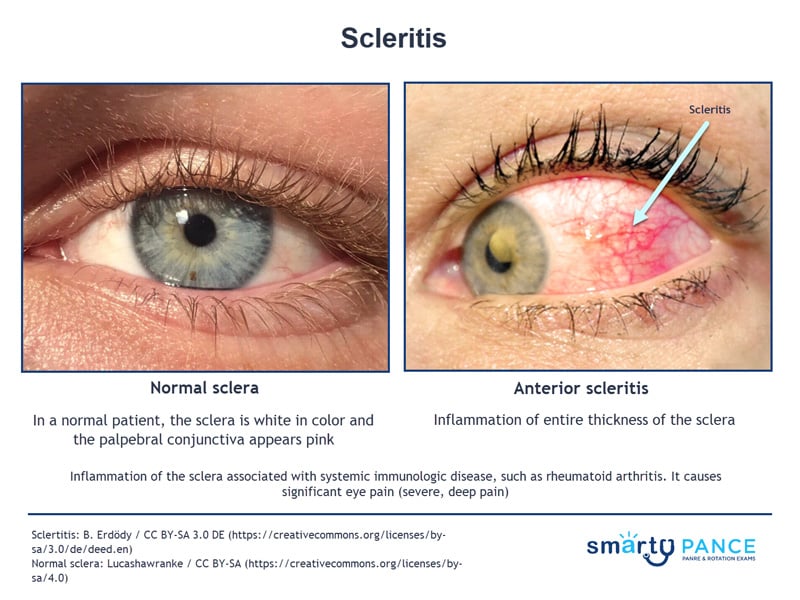
| Inflammation of the iris and ciliary body | Inflammation of the sclera | Inflammation of the uveal tract (iris, ciliary body, choroid) |
| Autoimmune: Ankylosing spondylitis, reactive arthritis, sarcoidosis
Infectious: HSV, syphilis, TB |
Autoimmune: Rheumatoid arthritis, lupus, granulomatosis with polyangiitis | Autoimmune: Ankylosing spondylitis, reactive arthritis, IBD (HLA-B27)
Infectious: HSV, CMV, syphilis, TB |
| Eye pain, redness (ciliary flush), photophobia, blurred vision, small irregular pupil | Severe deep eye pain worsened by eye movement, redness, tenderness on palpation | Anterior: Pain, photophobia, redness
Posterior: Painless vision loss, floaters |
| Slit-lamp: Cells and flare in anterior chamber, keratic precipitates | Clinical exam: Diffuse scleral redness, tender globe; slit-lamp confirms scleral inflammation | Slit-lamp: Cells/flare (anterior), vitritis/choroiditis (posterior), keratic precipitates; Labs (HLA-B27, infectious screens) |
| Topical corticosteroids, cycloplegics, ophthalmology referral, systemic workup if recurrent | Systemic NSAIDs (e.g., indomethacin), corticosteroids/immunosuppressants, ophthalmology & rheumatology referral | Anterior: Topical steroids, cycloplegics
Posterior: Systemic steroids/immunosuppressants, treat underlying cause |
| Posterior synechiae, glaucoma, vision loss | Vision impairment, scleral thinning/perforation | Glaucoma, cataracts, permanent vision loss |
| Iritis | Patient will present as → a 32-year-old woman with a history of ankylosing spondylitis presenting with redness, eye pain, and photophobia in the right eye. She denies trauma or discharge but reports blurry vision. On examination, her right eye has a circumferential redness near the corneal limbus (ciliary flush), a small, irregularly shaped pupil, and cells and flare in the anterior chamber on slit-lamp examination. Iritis (anterior uveitis) is suspected, and she is urgently referred to an ophthalmologist for evaluation and management. Iritis (anterior uveitis) is an inflammation of the iris, commonly associated with autoimmune diseases or infections, leading to ocular pain and visual impairment
DX: Diagnosis is clinical, often confirmed by slit-lamp examination showing inflammation in the anterior chamber (e.g., cells and flare) TX: Referral to an ophthalmologist is essential for proper diagnosis and management
|
| Scleritis | Patient will present as → a 42-year-old female with rheumatoid arthritis presents with deep, aching pain in her right eye, worsening with movement, along with redness and blurred vision. Examination reveals diffuse redness involving the sclera with tenderness on palpation. Slit-lamp exam confirms scleral inflammation, consistent with diffuse anterior scleritis. Management includes systemic NSAIDs (e.g., indomethacin) and referral to a rheumatologist for possible immunosuppressive therapy. Follow-up with ophthalmology is necessary to monitor for complications. Inflammation of the sclera (the white outer coating of the eye) associated with systemic immunologic disease, such as rheumatoid arthritis
DX: On examination, there is ocular redness and pain on palpation of the eyeball. It can cause visual impairment
TX: Refer the patient for prompt evaluation by an ophthalmologist
|
| Uveitis | Patient will present as → a 32-year-old male presents with eye pain, redness, and blurred vision in his left eye for three days, along with photophobia and mild tearing. He reports chronic lower back pain that improves with activity. Exam reveals ciliary injection, a small, irregular pupil, and anterior chamber inflammation with keratic precipitates on slit-lamp examination. He is diagnosed with anterior uveitis, likely related to HLA-B27 seronegative spondyloarthropathy. Management includes topical corticosteroids, cycloplegics, and rheumatology referral. Follow-up is arranged to monitor for recurrence and complications. Uveitis is inflammation of the uveal tract (iris, ciliary body, choroid) and can be associated with autoimmune, infectious, or idiopathic causes.
Causes include autoimmune (ankylosing spondylitis, reactive arthritis, IBD – HLA-B27), infectious (HSV, CMV, syphilis, TB), or idiopathic. Anterior uveitis presents with eye pain, photophobia, redness, blurred vision; posterior with painless vision loss and floaters. DX:
TX:
Complications: If untreated, can lead to glaucoma, cataracts, permanent vision loss
|
{kind=link}