

18 y/o with facial and eyelid trauma after an MVA
Patient with ocular foreign body will present as → a 33-year-old complaining of right eye pain and irritation. He states that he wasn't wearing glasses, and while trimming his driveway with his weed trimmer, "something flew into my eye." Visual acuity is 20/20. Pupils are equal, round, reactive to light, and accommodation. Extraocular movements are intact. On physical examination, you note a tearing, red, and severely painful right eye. Fluorescein staining shows a linear corneal abrasion with no evidence of a penetrating injury. The patient is diagnosed with a corneal foreign body. Management includes removal of the foreign body using a sterile cotton swab under topical anesthesia, initiation of topical erythromycin ointment, and follow-up in 24-48 hours to ensure proper healing.
Alternatively:
Patient with chemical injury will present as → a 45-year-old woman presents after accidentally splashing household cleaning solution in her eyes. She reports severe burning pain, tearing, and blurred vision. On examination, the eye appears red with diffuse conjunctival injection. A pH test of the eye reveals an alkaline pH of 9, confirming a chemical injury. Emergent irrigation is performed.
An ocular foreign body is any object embedded in or adhering to the conjunctiva or cornea in addition, chemical injuries involve exposure to caustic substances
- Symptoms include pain, tearing, redness, blurred vision, and a sensation of something in the eye; chemical injuries may also present with burning, photophobia, and blepharospasm
- Metallic foreign bodies may leave a rust ring
- A foreign body trapped under the upper lid may cause one or more vertical corneal abrasions that worsen as a result of blinking
- Intraocular penetration can occur with seemingly minor trauma, particularly when foreign bodies result from high-speed machines (e.g., drills, saws, anything with a metal-on-metal mechanism), hammering, or explosions
- If you can't remove the foreign body easily, then refer to the ophthalmologist
- For chemical injuries, alkaline substances (e.g., lye, ammonia) cause more severe damage than acids due to deeper tissue penetration
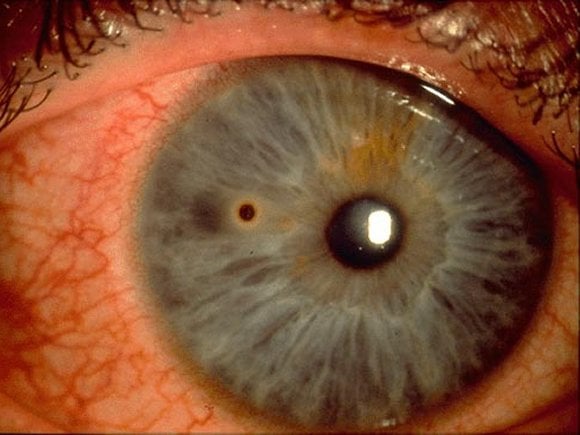
Corneal metallic foreign body with a "rust ring."
Slit-lamp examination, usually with fluorescein staining with cobalt light illumination, renders abrasions and nonmetallic foreign bodies more apparent
- Eversion of the eyelid to inspect for hidden foreign bodies
- pH testing of the ocular surface for chemical injuries
- X-ray or CT may be necessary if there is evidence of penetration of the globe
Superficial foreign bodies can be removed with irrigation or a sterile cotton swab after the installation of a topical anesthetic
- Embedded foreign bodies may require removal with a sterile needle or ophthalmic burr under magnification
- For chemical injuries—immediate irrigation with copious amounts of sterile saline or water for at least 15-30 minutes until the pH normalizes
- Topical antibiotics (e.g., erythromycin ointment) should be prescribed to prevent infection after removal
- Referral to ophthalmology is necessary for large, deeply embedded, or suspected penetrating injuries
- Preventive measures include wearing protective eyewear during activities with a high risk of exposure
- Patients should be educated to avoid rubbing the eye, which can exacerbate injury
- Patients with uncomplicated, small, traumatic, or foreign body corneal abrasions should NOT undergo patching
- Tetanus prophylaxis should be updated if necessary
Intraocular foreign bodies—inside the eye, penetrating the cornea, sclera, or lodged within internal ocular structures (e.g., anterior chamber, vitreous) require immediate surgical removal by an ophthalmologist
- Systemic and topical antimicrobials (effective against Bacillus cereus if the injury involved contamination with soil or vegetation) are indicated
Rust ring—After a foreign body containing iron is removed, there is often a residual rust ring and reactive infiltrate. Patients with rust rings should be treated as patients with corneal abrasions. The rust ring itself is not harmful and will usually resorb gradually.
Question 1 |
MRI Hint: MRI should never be used when there is suspicion of an iron-containing intraocular foreign body. | |
X-ray orbits | |
Applanation tonometry Hint: Tonometry is used to evaluate intraocular pressure, but not the presence of intraocular foreign bodies. | |
Fluorescein angiography Hint: Fluorescein angiography is used to evaluate vessels of the eye, not intraocular foreign bodies. |
Question 2 |
Check visual acuity Hint: Delaying irrigation of the eye to assess vision or corneal damage is inappropriate as damage to the eye may occur during the delay. | |
Flush the eye with two liters saline | |
Check for corneal damage with fluorescein Hint: See A for explanation. | |
Instill a topical anesthetic to facilitate examination Hint: Topical anesthetic may be used to facilitate irrigation with a Morgan lens, but see A for explanation. |
Question 3 |
irrigate the eye for at least 20 minutes | |
apply Bacitracin ointment and patch the eye Hint: See A for explanation. | |
remove the sparkle with a moistened cotton swab Hint: See A for explanation. | |
protect the eye with a metal shield and refer to an eye ophthalmologist Hint: See A for explanation. |
Question 4 |
Administer tetanus Hint: Tetanus booster is only required every 5 years. | |
Prescribe Tetracaine ophthalmic Hint: See D for explanation. | |
Provide reassurance only Hint: See D for explanation. | |
Refer to ophthalmologist |
|
List |
References: Merck Manual · UpToDate