NCCPA™ PANCE EENT Content Blueprint ⇒ ear disorders ⇒ hearing impairment

To watch this and all of Joe Gilboy PA-C's video lessons, you must be a member. Members can log in here or join now.
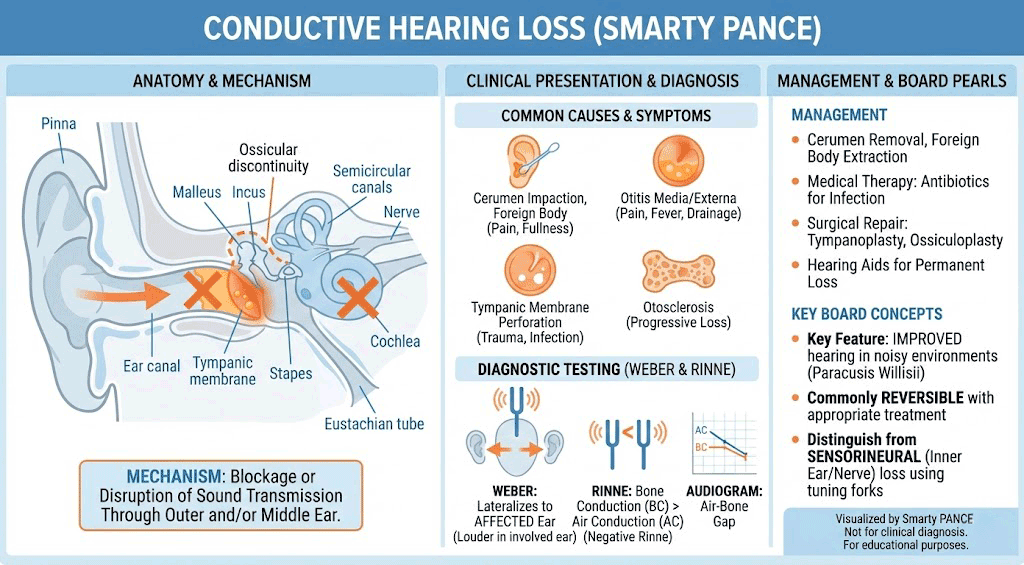
Conductive vs. Sensorineural Hearing Loss
| Feature | Conductive Hearing Loss (CHL) | Sensorineural Hearing Loss (SNHL) |
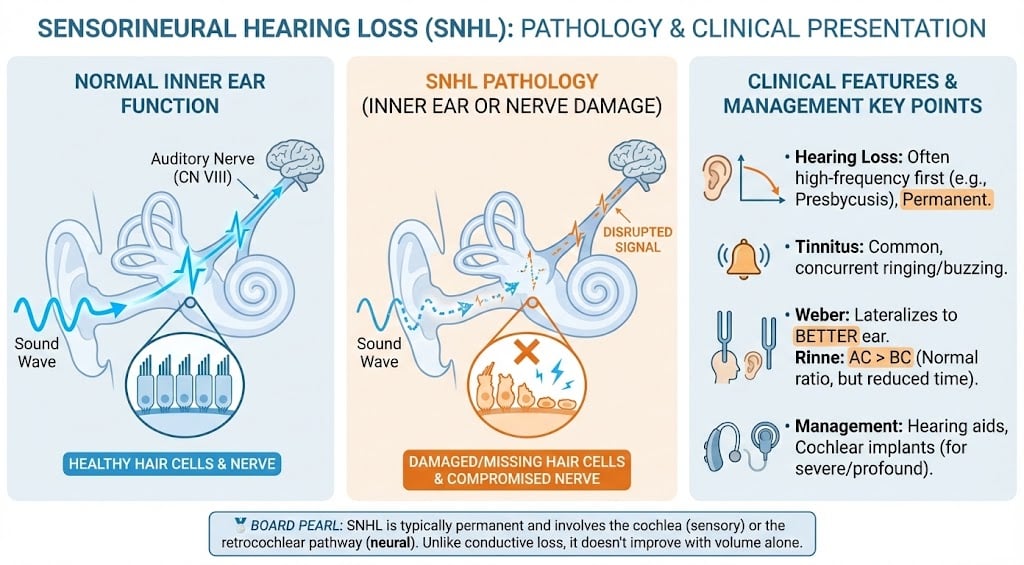
| Pathophysiology | Problem with the "Hardware" (External/Middle ear). Sound can’t get in. | Problem with the "Software" (Inner ear/CN VIII). Sound can’t be processed. |
| Common Causes | Wax (cerumen), fluid (Otitis Media), hole in drum (TM perforation), stuck bones (Otosclerosis). | Aging (Presbycusis), loud music, Meniere’s, Acoustic Neuroma. |
| Weber Test | Localizes to AFFECTED ear (The "noisy room" effect—the bad ear hears the vibration better). | Localizes to UNAFFECTED ear (The good ear is the only one with a working nerve). |
| Rinne Test | Bone > Air (Negative). The "shortcut" through the bone works better than the broken "main road." | Air > Bone (Normal/Positive). Both are reduced, but the ratio stays the same. |
| Audiogram | Air-Bone Gap. Bone conduction is normal, but Air conduction is low. | No Gap. Both Air and Bone conduction are equally poor. |
| Speech Clarity | Sounds are Muffled (Volume problem). Clarity is okay if loud enough. | Sounds are Distorted (Quality problem). Turning it up just makes it "loud and fuzzy." |
| Treatment | Often fixable (Surgery, cleaning, or antibiotics). | Often permanent (Hearing aids or Cochlear implants). |
| Conductive Hearing Impairment | Patient will present as → a 27-year-old male presents with left-sided hearing loss and ear fullness two weeks after a cold. Exam reveals a dull, retracted tympanic membrane with air-fluid levels. Weber test lateralizes to the left, and Rinne shows BC > AC, consistent with conductive hearing loss. Tympanometry confirms middle ear effusion. Diagnosis is serous otitis media. Management is conservative, as many cases resolve spontaneously. He is advised on autoinsufflation (e.g., Valsalva maneuver) to help equalize pressure and is instructed to avoid swimming or air travel until symptoms resolve. Nasal corticosteroids or decongestants may be considered if congestion is contributing. Follow-up is scheduled in 4–6 weeks. If effusion persists or worsens, audiology referral and possible ENT evaluation for tympanostomy tubes will be considered.
Conductive Hearing Impairment occurs when sound transmission is blocked in the external or middle ear, preventing sound from reaching the inner ear.
DX: Diagnosis is clinical and confirmed with otoscopic exam, audiometry, and possibly tympanometry
TX: Management depends on the cause:
Prognosis is generally good, especially when the underlying cause is treated or corrected early |
| Sensorineural Hearing Loss | Patient will present as → a 67-year-old male presents with gradual bilateral hearing loss over one year, especially in noisy environments. He worked in a loud factory for 30+ years without hearing protection. Otoscopy is normal. Rinne is positive bilaterally, and Weber lateralizes to the right, consistent with sensorineural hearing loss. Audiometry confirms high-frequency bilateral sensorineural loss, consistent with presbycusis. Management includes referral for hearing aids, hearing protection counseling, and routine audiologic monitoring.
Sensorineural Hearing Loss (SNHL) is caused by damage to the inner ear (cochlea) or the auditory nerve, resulting in permanent hearing impairment
Presbycusis results from progressive degeneration of cochlear hair cells, the stria vascularis, and auditory neurons due to aging, leading to impaired high-frequency sound transduction and gradual bilateral sensorineural hearing loss.
DX: Diagnosis confirmed with audiometry, which shows elevated thresholds for air and bone conduction with no air-bone gap
TX: Treatment depends on the cause and severity:
Prognosis varies—SNHL is typically irreversible, but early intervention can improve communication and quality of life |
Question 1 |
The tympanic membrane is movable with pneumatic otoscopy Hint: A movable tympanic membrane indicates there is no effusion, and is not the Weber test. | |
The tympanic membrane is pearly gray with a sharp cone of light with apex at the umbo Hint: The tympanic membrane is evaluated by direct observation with an otoscope, and is not the Weber test. | |
Sound is heard equally in both ears when a vibrating tuning fork is placed on the mid forehead | |
Air conduction is greater than bone conduction when a vibrating tuning fork is moved from the mastoid bone to close to the ear canal Hint: A normal Rinne test means that tuning fork vibration is heard longer through the air than the bone. |
Question 2 |
auditory brainstem evoked response Hint: See B for explanation. | |
gadolinium-enhanced MRI | |
acoustic reflex testing Hint: See B for explanation. | |
vestibular testing Hint: Vestibular testing is not a useful screening test for acoustic neuromas. |
Question 3 |
otosclerosis Hint: See C for explanation. | |
cholesteatoma Hint: See C for explanation. | |
impacted cerumen | |
chronic serous otitis media Hint: See C for explanation. |
Question 4 |
audiometry Hint: Pure tone audiometry can be used to screen for hearing deficits in children over the age of 3 years. | |
tympanometry Hint: Tympanometry is used to identify an effusion as the cause of hearing loss, but in infants over the age of months. | |
acoustic reflectometry Hint: Acoustic reflectometry measures the spectral gradient of the tympanic membrane, but is not used clinically due to concerns about its reliability. | |
auditory-evoked potentials |
Question 5 |
Sounds best heard in the left ear on Weber test. | |
Air conduction longer than bone conduction in the left ear on Rinne test. Hint: With conductive hearing loss, bone conduction should be heard as long as or longer than air conduction of sound in the effected ear. Air conduction lasting longer than bone conduction of sound would indicate sensorineural hearing loss. | |
Sound best heard in the right ear on Weber test. Hint: Sound best heard in the ear with unaffected hearing on Weber test (in this case, the right ear) is indicative of sensorineural hearing loss. | |
Bone conduction longer than air conduction in the right ear. Hint: With conductive hearing loss, bone conduction should be heard as long as or longer than air conduction of sound in the affected ear. The right ear showed normal hearing on physical exam. |
Question 6 |
referred to the right ear | |
referred to the left ear Hint: See A for explanation. | |
equal in both ears Hint: See A for explanation. | |
louder with air conduction Hint: Bone conduction as noted with the Rinne test is louder than air with conductive hearing loss. |
Question 7 |
Advise him to discontinue use of cotton swabs | |
Encourage jet irrigator (i.e. WaterPik) to clean ears Hint: Use of jet irrigators designed for cleaning teeth (i.e. waterPik) for wax removal should be avoided since they may result in tympanic membrane perforations. | |
Instruct in ear irrigation with cold water Hint: Irrigation is performed with water at body temperature to avoid a vestibular caloric response. | |
Refer to dermatologist Hint: See A for explanation. |
|
List |