Patient will present as → a 4-year-old girl who is brought to the clinic by her mother, who states that the child has been complaining of progressively worsening ear pain and itchiness over the past week. Examination reveals left tragal tenderness and an edematous and closed canal. Weber lateralizes to the left.
 Otitis externa (aka swimmer's ear) is an infection of the external auditory canal secondary to trauma or a consistently moist environment, which favors the growth of fungi or bacteria
Otitis externa (aka swimmer's ear) is an infection of the external auditory canal secondary to trauma or a consistently moist environment, which favors the growth of fungi or bacteria
- It generally presents with canal itching and pain with movement of the ear. If the canal is closed, Weber is expected to lateralize to the side of the blocked canal
- Painful edema with cheesy white discharge, sometimes it is impossible to see the TM
- Most common causes: Pseudomonas aeruginosa (38%), S. epidermidis (9 percent), and Staphylococcus aureus (8 percent)
- Malignant otitis externa is commonly seen in diabetics
- Fungal OM is responsible for approximately 9 percent of ear canal infections. Aspergillus niger (90%) and Candida are the most common organisms
Diagnosis is clinical by otoscopy

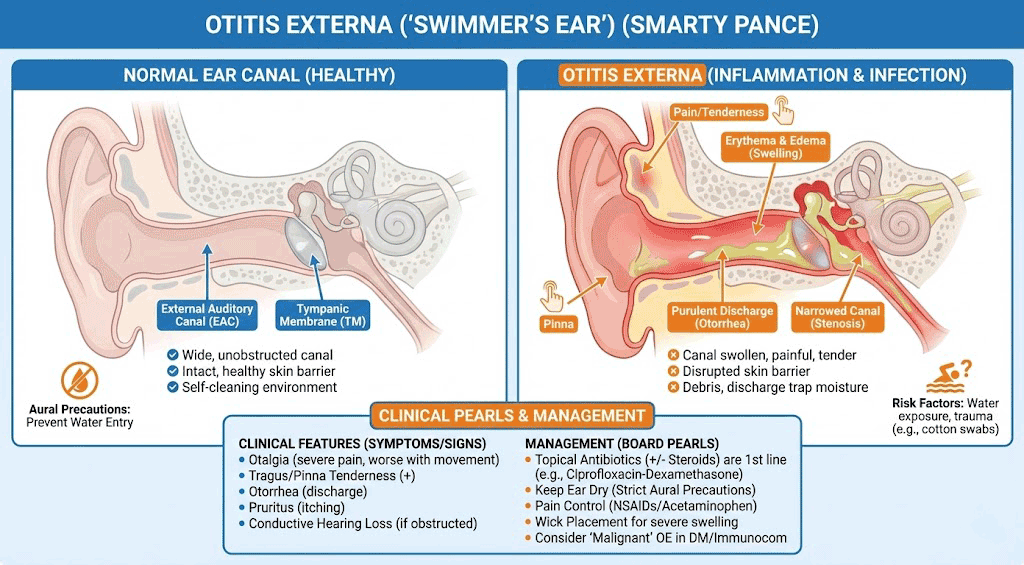
Otitis externa (“swimmer’s ear”) with inflammation and narrowing of the external auditory canal. Photo by James Heilman, MD via Wikimedia Commons, CC BY 3.0.
Bacterial otitis externa:
- If perforated or chance of perforation: Ciprofloxacin 0.3% and dexamethasone 0.1% suspension: 4 drops BID × 7 days or ofloxacin: 0.3% solution 10 drops once a day × 7 days
- Cortisporin otic SUSPENSION, which is less irritating than the solution
Fungal otitis externa
- Topical therapy, anti-yeast for Candida or yeast: 2% acetic acid 3–4 drops QID; clotrimazole 1% solution; itraconazole oral
- Step 1: Can the tympanic membrane (TM) be visualized and is it intact?
→ Yes: Use neomycin/polymyxin B/hydrocortisone otic suspension
→ No or TM is perforated/tubes present: Use ofloxacin or ciprofloxacin otic or ophthalmic drops (non-ototoxic and sterile) - Step 2: Is cost a concern and TM is intact?
→ Yes: Consider gentamicin or tobramycin ophthalmic drops (low-cost alternative, only if TM is intact)
→ No: Use Ciprodex (ciprofloxacin/dexamethasone) for faster symptom relief - Step 3: Is the canal too swollen for drop entry?
→ Yes: Insert wick to facilitate medication delivery
→ No: Proceed with drop instillation - Step 4: Pain management
→ Use oral acetaminophen or ibuprofen
→ Avoid topical analgesics - Step 5: Prevent recurrence
→ Recommend drying ears after water exposure (hairdryer or 1:1 vinegar-alcohol mix)
Question 1 |
Staphylococcus aureus Hint: While S. aureus can cause otitis externa, it is less common than Pseudomonas aeruginosa. S. aureus is more commonly associated with skin infections, such as impetigo or folliculitis. | |
Pseudomonas aeruginosa | |
Candida albicans Hint: Candida albicans is a yeast that can cause fungal otitis externa, particularly in individuals with immunocompromised states or those using hearing aids. However, fungal infections are less common than bacterial infections. | |
Streptococcus pneumoniae Hint: Streptococcus pneumoniae is a common cause of otitis media, not otitis externa. It is associated with middle ear infections rather than infections of the external ear canal. | |
Aspergillus niger Hint: Aspergillus niger is another fungal cause of otitis externa but is much less common than Pseudomonas aeruginosa. It typically occurs in immunocompromised individuals or those with chronic otitis externa. |
Question 2 |
Oral amoxicillin Hint: Amoxicillin is typically used for otitis media, not otitis externa. Moreover, it is not the first-line treatment for otitis externa, particularly when Pseudomonas aeruginosa, a common pathogen in otitis externa, is suspected. | |
Topical ofloxacin ear drops | |
Topical neomycin/polymyxin B/hydrocortisone ear drops Hint: These drops are generally effective for otitis externa, but they are contraindicated in the presence of a perforated tympanic membrane because neomycin is ototoxic and could potentially cause hearing loss if it enters the middle ear through the perforation. | |
Topical acetic acid solution Hint: Acetic acid can be used in cases of mild otitis externa to restore the normal acidic environment of the ear canal, but it is not effective for treating an infection with a suspected ruptured tympanic membrane and should be avoided in such cases due to the risk of ototoxicity. | |
Oral ciprofloxacin Hint: While ciprofloxacin is effective against Pseudomonas aeruginosa, systemic antibiotics are generally not needed for uncomplicated otitis externa unless there is systemic involvement, significant surrounding tissue infection, or the patient is immunocompromised. |
Question 3 |
Continue prophylactic antibiotics for an additional 6 weeks Hint: See C for explanation. | |
Immediately discontinue antibiotics Hint: See C for explanation. | |
Obtain gallium scan to ensure reduction of inflammatory process | |
Skin swab culture of healthy tissue Hint: See C for explanation. |
Question 4 |
Oral antibiotics and observation Hint: Oral antibiotics alone are not sufficient in the treatment of mastoiditis, especially in the presence of systemic symptoms and radiographic evidence of mastoid involvement. This approach would risk further complications, including the spread of the infection. | |
High-dose intravenous antibiotics and myringotomy | |
Tympanostomy tube placement Hint: While tympanostomy tube placement may be considered in recurrent otitis media, it is not the initial treatment for acute mastoiditis. The priority in this case is to control the infection aggressively with intravenous antibiotics and possibly surgical drainage. | |
Surgical mastoidectomy Hint: Surgical mastoidectomy may be required if the infection does not respond to intravenous antibiotics and myringotomy or if there is evidence of complications such as abscess formation. However, it is not the first-line treatment and is reserved for cases where initial management fails. | |
Oral corticosteroids Hint: Oral corticosteroids are not indicated in the management of mastoiditis and could potentially worsen the infection by suppressing the immune response. The primary treatment involves controlling the infection with antibiotics and surgical intervention if necessary. |
|
List |
References: Merck Manual · UpToDate