 Lecture
Lecture


55 y/o male with dizziness
Patient will present as → a 29-year-old male with intense nausea and vomiting that began yesterday. He states that he ran a 5K race in the morning and felt well while resting afterward. However, when he arose, he experienced two episodes of emesis accompanied by a sensation that the world was spinning around him. This lasted about one minute and subsided. He denies tinnitus or hearing changes but feels imbalanced. He has a PMH of migraines, but he typically does not have nausea or vomiting with migraine episodes. His temperature is 98.7°F, blood pressure is 132/82 mmHg, pulse is 75/min, and respirations are 13/min. The cardiopulmonary exam is unremarkable. Cranial nerves are intact, and gross motor function and sensation are within normal limits. When the patient’s head is turned to the right side and lowered quickly to the supine position, he claims that he feels “dizzy and nauseous.” Nystagmus is noted in both eyes.

To watch this and all of Joe Gilboy PA-C's video lessons, you must be a member. Members can log in here or join now.
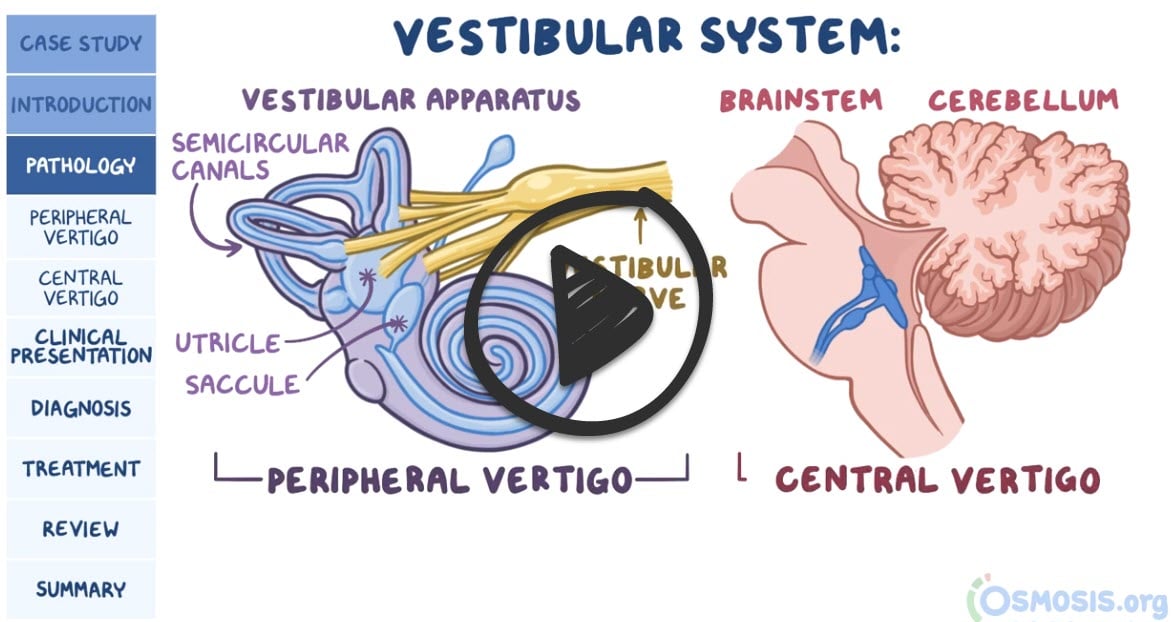
Vertigo is the sensation of movement (spinning, tumbling, or falling) in the absence of any actual movement or an over-response to movement.
- Peripheral (inner ear) causes of vestibular dysfunction include labyrinthitis, benign paroxysmal positional vertigo, Ménière syndrome, vestibular neuritis, and head injury
- Central (neurologic) causes of vertigo include brainstem vascular disease, arteriovenous malformations, tumors, multiple sclerosis, and vertebrobasilar migraine
Duration and presence of hearing loss/nystagmus can help with the diagnosis
- Peripheral vertigo is associated with sudden onset, nausea/vomiting, tinnitus, hearing loss, and nystagmus (typically horizontal with a rotatory component)
- Central vertigo is associated with a more gradual onset and vertical nystagmus. Unlike peripheral vertigo, it does not present with auditory symptoms. Central vertigo is commonly associated with motor, sensory, or cerebellar deficits.
Vertigo and syncope = vertebrobasilar insufficiency
Differential Diagnosis of Peripheral Vertigo & Ear Disorders
| Disease | Pathophysiology & Characteristics | Symptoms | Diagnostic Test | Treatment |
| BPPV | Otoliths (crystals) displaced into semicircular canals; triggered by head movement. | Brief episodes of vertigo (seconds); No hearing loss or tinnitus. | Dix-Hallpike maneuver (observing nystagmus). | Epley maneuver (canalith repositioning); Meclizine is rarely effective. |
| Vestibular Neuritis | Inflammation limited to the vestibular nerve (the part of CN VIII responsible for balance); often follows viral URI. | Single acute episode of continuous vertigo; No hearing loss or tinnitus. | Clinical diagnosis; Head-impulse test. | Supportive (Meclizine, anti-emetics); Steroids. |
| Labyrinthitis | Inflammation affects the entire labyrinth (the "room" that houses both balance organs and the cochlea); often post-viral. | Continuous vertigo PLUS hearing loss and tinnitus. | Clinical diagnosis; Audiometry. | Meclizine + Steroids; Antibiotics if bacterial. |
| Meniere’s Disease | Endolymphatic hydrops (increased fluid pressure in the inner ear). | Episodic vertigo (hours), fluctuating hearing loss, tinnitus, and ear fullness. | Clinical; Audiometry shows low-frequency loss. | Low-salt diet, avoid caffeine/alcohol/nicotine, Diuretics. |
| Acoustic Neuroma | Benign tumor on CN VIII; associated with NF2 if bilateral. | Progressive unilateral hearing loss, tinnitus, ataxia, and facial numbness. | MRI of the Internal Auditory Canal (IAC). | Surgery or Radiation (Gamma Knife). |
Clinical features of peripheral versus central vertigo
| Peripheral | Central | |
| Nystagmus | ||
| Features (direction and type) | Unidirectional, fast component toward the normal ear; never reverses direction
Horizontal with a torsional component; never purely torsional or vertical |
Sometimes reverses direction when patient looks in the direction of slow component
Can be any direction; note that purely vertical or purely torsional nystagmus is a central sign |
| Effect of visual fixation | Suppressed | Not suppressed |
| Postural instability | Unidirectional instability, walking preserved | Severe instability, patient often falls when walking |
| Deafness or tinnitus | May be present | Usually absent |
| Other neurologic signs and symptoms | Absent | Often present (eg, diplopia, ataxia, dysarthria, dysphagia, focal or lateralized weakness) |
- With benign positional vertigo, the Dix–Hallpike maneuver (i.e., quickly turning the patient’s head 90 degrees while the patient is in the supine position) will produce delayed fatigable nystagmus (nystagmus abates when the provocative position is held for a long time)
- If the nystagmus is non-fatigable (not inhibited by fixation of gaze), a central cause for the vertigo is more likely
- Other testing, such as audiometry, caloric stimulation, electronystagmography (ENG), MRI, and evoked potentials, are indicated with persistent vertigo or with suspected central nervous system (CNS) involvement
- + Romberg Sign = central vertigo
Therapy is based on the underlying etiology
- Vestibular suppressants (i.e., diazepam, meclizine) may help with acute symptoms
- Benign paroxysmal positional vertigo may respond to physical therapy maneuvers (Epley Maneuver)
- Some cases may require interventional/surgical therapies
 Osmosis Osmosis |
|
 |
 Vertigo is defined as an illusion of movement that’s either self-movement or movement of the surrounding environment. Vertigo is classified into peripheral and central vertigo. Peripheral vertigo is caused by disorders like BPPV, vestibular neuritis, Ménière’s disease, and an acoustic neuroma, while the causes of central vertigo include posterior circulation stroke and brainstem or cerebellar tumors or lesions. A diagnosis can be made based on clinical presentation and patient’s history, but sometimes imaging studies should be done to rule out central causes like a posterior circulation stroke.
Vertigo is defined as an illusion of movement that’s either self-movement or movement of the surrounding environment. Vertigo is classified into peripheral and central vertigo. Peripheral vertigo is caused by disorders like BPPV, vestibular neuritis, Ménière’s disease, and an acoustic neuroma, while the causes of central vertigo include posterior circulation stroke and brainstem or cerebellar tumors or lesions. A diagnosis can be made based on clinical presentation and patient’s history, but sometimes imaging studies should be done to rule out central causes like a posterior circulation stroke.
| Vertigo | Play Video + Quiz |
| Meniere’s disease | Play Video + Quiz |
Question 1 |
Meniere's disease Hint: Meniere's disease involves episodic vertigo, hearing loss, tinnitus, and aural fullness. | |
Vestibular neuritis Hint: Vestibular neuritis presents with prolonged vertigo but not triggered by head movements, and without hearing loss. | |
Labyrinthitis Hint: Labyrinthitis includes vertigo and hearing loss, not solely provoked by position changes. | |
Benign paroxysmal positional vertigo | |
Acoustic neuroma Hint: Acoustic neuroma typically presents with progressive unilateral hearing loss and tinnitus, not episodic positional vertigo. |
Question 2 |
Benign paroxysmal positional vertigo Hint: BPPV causes brief episodes of vertigo related to head position changes. | |
Vestibular neuritis | |
Labyrinthitis Hint: Labyrinthitis also presents with auditory symptoms like hearing loss. | |
Meniere's disease Hint: Meniere's disease involves episodic vertigo, hearing loss, tinnitus, and aural fullness. | |
Acoustic neuroma Hint: Acoustic neuroma usually presents with unilateral hearing loss and tinnitus, not acute vertigo. |
Question 3 |
Benign paroxysmal positional vertigo Hint: BPPV is characterized by brief, positionally triggered episodes of vertigo without hearing loss. | |
Vestibular neuritis Hint: Vestibular neuritis presents with vertigo but without hearing loss or tinnitus. | |
Labyrinthitis | |
Meniere's disease Hint: Meniere's disease involves episodic vertigo, not continuous, along with fluctuating hearing loss. | |
Acoustic neuroma Hint: Acoustic neuroma presents with progressive hearing loss and tinnitus, typically without acute vertigo episodes. |
Question 4 |
Benign paroxysmal positional vertigo Hint: BPPV involves short-lived vertigo episodes triggered by head movements, without auditory symptoms. | |
Vestibular neuritis Hint: Vestibular neuritis is marked by a single prolonged episode of vertigo without hearing loss. | |
Labyrinthitis Hint: Labyrinthitis presents with continuous vertigo and hearing loss, typically following an infection. | |
Meniere's disease | |
Acoustic neuroma Hint: Acoustic neuroma involves progressive unilateral hearing loss and tinnitus but not episodic vertigo. |
Question 5 |
Acoustic neuroma | |
Benign paroxysmal positional vertigo (BPPV) Hint: BPPV causes episodic vertigo without hearing loss or tinnitus. | |
Labyrinthitis Hint: Labyrinthitis includes vertigo and hearing loss but is not associated with a mass on imaging. | |
Meniere's disease Hint: Meniere's disease involves episodic vertigo and hearing loss but not due to a cerebellopontine angle mass. | |
Vestibular neuritis Hint: Vestibular neuritis presents with acute vertigo but no hearing loss. |
|
List |
References: Merck Manual · UpToDate