Patient will present as → a 33-year-old male presents to the emergency department with a 3-day history of severe throat pain, fever, and difficulty swallowing. He mentions that the pain has progressively worsened, now radiating to his ear, and describes a feeling of tightness and swelling in his neck. He also reports a muffled voice and difficulty breathing, particularly when lying down. His medical history is notable for untreated dental caries and a recent upper respiratory tract infection. On examination, he is febrile with a temperature of 39.2°C (102.6°F). Inspection of the oropharynx is limited due to trismus. There is noticeable swelling and tenderness to palpation on the left side of his neck, with overlying erythema and warmth. His voice is hoarse, and he appears to be in respiratory distress with stridor noted on auscultation. Laboratory tests reveal leukocytosis. A CT scan of the neck with contrast shows a large abscess in the left parapharyngeal space with surrounding cellulitis, consistent with a deep neck infection. The patient is admitted to the intensive care unit for airway monitoring given his respiratory distress. Immediate intravenous broad-spectrum antibiotics are initiated, and an urgent otolaryngology consultation is obtained for possible surgical drainage. He is also evaluated by a dentist for management of his dental caries, which is suspected to be the source of the infection.
Deep neck infections are serious bacterial infections of the deep cervical fascia spaces, including the parapharyngeal, retropharyngeal, and submandibular spaces
- Common causes include dental infections (e.g., peritonsillar abscess, Ludwig's angina), tonsillitis, pharyngitis, and trauma (e.g., foreign bodies, recent surgery)
- Symptoms include fever, neck pain/swelling, trismus (difficulty or inability to open the mouth), dysphagia, odynophagia (pain with swallowing), muffled voice, and respiratory distress
- Staphylococcus aureus is the most common cause of deep neck infections in immunocompetent individuals
- Complications include airway obstruction, mediastinitis, sepsis, jugular vein thrombosis (Lemierre’s syndrome), and carotid artery erosion

Minor trauma triggering cervicofacial necrotizing fasciitis from an odontogenic abscess. Image by Jain S, Nagpure PS, Singh R, Garg D - CC 2.0
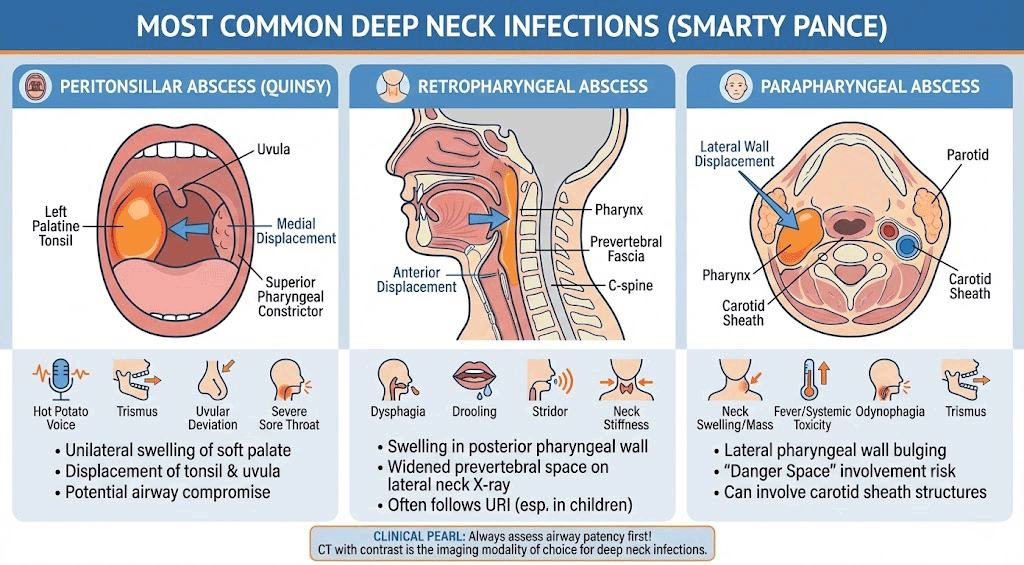
Here is a table summarizing the most common deep neck infections, including their locations, common causes, and symptoms:
| Infection | Location | Common Causes | Symptoms/Signs |
| Peritonsillar Abscess | Around the tonsils | Streptococcus pyogenes, Staphylococcus aureus, anaerobes | Severe sore throat, difficulty swallowing, fever, "hot potato" voice
Uvular deviation to the contralateral tonsillar pillar |
| Retropharyngeal Abscess | Retropharyngeal space, behind the pharynx | Streptococcus pyogenes, Staphylococcus aureus, anaerobes | Fever, neck stiffness, sore throat, difficulty swallowing, respiratory distress
Midline uvula Widening of prevertebral space on lateral neck radiograph |
| Parapharyngeal Abscess | Parapharyngeal space, lateral to the pharynx | Streptococcus species, Staphylococcus aureus, anaerobes | Fever, trismus (lockjaw), neck pain, swelling |
| Ludwig's Angina | Submandibular space, beneath the floor of the mouth | Streptococcus species, Staphylococcus aureus, anaerobes | Rapidly progressing cellulitis, swelling, pain in the floor of the mouth, difficulty swallowing, potentially compromised airway |
| Suppurative Lymphadenitis | Lymph nodes in the neck | Streptococcus pyogenes, Staphylococcus aureus | Swollen, tender lymph nodes, fever, sometimes drainage of pus |
| Necrotizing Fasciitis | Fascia and subcutaneous tissues in the neck | Polymicrobial, including Group A Streptococcus, anaerobes | Severe pain, rapid progression, fever, signs of systemic toxicity |
| Lemierre's Syndrome | Jugular vein thrombophlebitis, often secondary to oropharyngeal infection | Fusobacterium necrophorum | Sore throat, fever, neck swelling, septic emboli leading to potential systemic complications like lung abscesses |
Computed tomography (CT) with contrast is the imaging modality of choice for the diagnosis of deep neck space infection
- MRI is useful for assessing the extent of soft tissue involvement and for delineating vascular complications
- Plain radiography is of limited utility for the evaluation of deep neck space infection
- Ultrasound may help detect superficial abscesses but is not useful for deeper infections
- Laboratory findings include elevated WBC count, CRP, and blood cultures

Large retropharyngeal abscess on CT

A lateral x-ray demonstrating prevertebral soft tissue swelling (marked by the arrow) as seen in a person with a retropharyngeal abscess.
The most common organisms isolated from deep neck space infections are staphylococcus aureus, including MRSA (22.5%), followed by streptococcus species (20%)
- For deep neck space infections that involve a drainable collection, aspiration or surgical drainage should be performed
- Antibiotic treatment depends on the location of infection - options include nafcillin, vancomycin, ciprofloxacin, etc.
- For parapharyngeal, retropharyngeal, or prevertebral space infections, therapy should generally be continued for two to three weeks
Question 1 |
A 35-year-old man presents to the emergency department with swelling on the right side of his neck and difficulty swallowing that has worsened over the last two days. He recently had a toothache in the lower right jaw but didn't go to the dentist. He is febrile with a temperature of 102.3°F. Which of the following is the most likely predisposing factor for this patient's condition?
Recent strep throat Hint: While strep throat can occasionally lead to complications such as peritonsillar abscess, it is less likely to be directly involved in the development of deep neck space infections. | |
History of head and neck cancer Hint: Head and neck cancer, and its treatments (radiation), can make individuals more susceptible to infections, but are not the primary driver for an otherwise healthy individual to develop a deep neck infection. | |
Recent upper respiratory infection Hint: Recent upper respiratory infection: Upper respiratory infections are common but they typically don't lead to complications involving deep neck spaces. | |
Dental caries | |
Chronic sinusitis Hint: Chronic sinusitis can involve adjacent structures, but deep neck infections usually stem from oral or pharyngeal sources.
|
Question 2 |
Group A streptococcus Hint: Less common cause than S. aureus in deep neck infections. | |
Staphylococcus aureus | |
Haemophilus influenzae Hint: Uncommon cause in adults without risk factors. | |
Mycobacterium tuberculosis Hint: Atypical cause in immunocompetent patients. | |
Actinomyces species Hint: Unusual cause of deep neck infections. |
Question 3 |
Lateral neck X-ray Hint: May show some abnormalities but lacks the detail of CT scans for diagnosing deep neck infections. | |
Contrast-enhanced CT scan of the neck | |
MRI of the neck Hint: Provides excellent soft tissue contrast but is less accessible and more time-consuming than CT, making it less ideal for initial assessment. | |
Ultrasound of the neck Hint: Useful for evaluating superficial structures but may not adequately visualize deep neck spaces. | |
Direct laryngoscopy Hint: Invasive and not the first-line diagnostic tool for deep neck infections; more useful for assessing airway patency and involvement. |
Question 4 |
Cephalexin Hint: A first generation cephalosporin that does not cover MRSA. | |
Clindamycin Hint: Active against MRSA but resistance is possible. | |
Amoxicillin Hint: A penicillin without MRSA coverage. | |
Vancomycin | |
Azithromycin Hint: A macrolide antibiotic that does not treat MRSA. |
|
List |
References: Merck Manual · UpToDate