Patient will present as → an 82-year-old man presents to the emergency department complaining of vision loss in his left eye. He states that it suddenly appeared as if a curtain was coming down over his left eye. It resolved after five minutes, and his vision returned to normal. He has a history of coronary artery disease and type 2 diabetes.
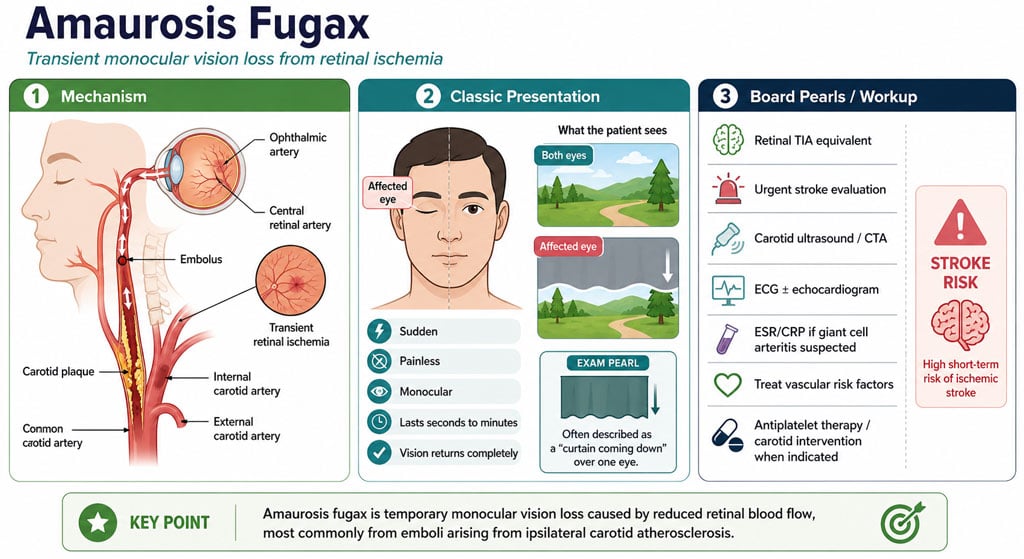
Amaurosis fugax (amaurosis meaning darkening, dark, or obscure, fugax meaning fleeting) is a painless temporary loss of vision in one or both eyes
- Amaurosis fugax is not itself a disease. Instead, it is a sign of other disorders.
- Other descriptions of this experience include monocular blindness, dimming, fogging, or blurring
Five distinct classes based on their supposed cause: embolic, hemodynamic, ocular, neurologic, and idiopathic
- Embolic/hematologic causes of amaurosis fugax:
- Most episodes of amaurosis fugax are the result of stenosis or atherosclerosis of the ipsilateral carotid artery
-
- The most common source of these emboli is an atherosclerotic carotid artery
- Amaurosis fugax (an example of a TIA) occurs if the clot passes and the vision loss is transient. If the clot cannot pass, central retinal artery occlusion occurs
- Other causes in this class include hypercoagulability states, thrombocytosis, SLE, and giant cell arteritis
- Ocular causes of amaurosis fugax include keratitis and posterior vitreous detachment
- Neurologic causes of amaurosis fugax include migraine, tumor, optic neuritis, and multiple sclerosis
- Idiopathic: despite extensive workups, a cause will not be found in some patients
A diagnostic evaluation should begin with the patient's history, followed by a physical exam, with particular importance being paid to the ophthalmic examination with regard to signs of ocular ischemia
- When investigating amaurosis fugax, an ophthalmologic consult is absolutely warranted if available
- Laboratory tests should also be ordered to investigate some of the more common systemic causes, including a CBC, ESR, lipid panel, EKG, and blood glucose level
- If laboratory tests are abnormal, a systemic disease process is likely, and if the ophthalmologic examination is abnormal, an ocular disease is likely
Noninvasive duplex ultrasound studies are recommended to identify carotid artery disease if ophthalmic and laboratory findings are inadequate for explanation
- Carotid imaging – Carotid duplex ultrasound, magnetic resonance angiography (MRA), or computed tomographic angiography should be ordered in all older patients (>50 years) and in younger patients with vascular risk factors (diabetes, hypertension, hyperlipidemia) who have experienced transient monocular visual loss (TMVL)
If the diagnostic workup reveals a systemic disease process, directed therapies to treat that underlying cause should be initiated
- If the amaurosis fugax is caused by an atherosclerotic lesion, aspirin is indicated, and carotid endarterectomy is considered based on the location and grade of the stenosis
- Left untreated, this event carries a high risk of stroke; after carotid endarterectomy, which has a low operative risk, there is a very low postoperative stroke rate
Question 1 |
Anterior cerebral Hint: Findings in ACA stroke may include the following: Disinhibition and speech perseveration. Primitive reflexes (eg, grasping, sucking reflexes) | |
Middle cerebral Hint: Blockage of the MCA results in deficits in movement and sensation (contralateral hemiplegia and hemianesthesia); difficulty swallowing (dysphagia); impaired speech ability (dysarthria, aphasia); and impaired vision and partial blindness (hemianopia); | |
Posterior cerebral Hint: Symptoms of posterior cerebral artery stroke include contralateral homonymous hemianopia (due to occipital infarction), hemisensory loss (due to thalamic infarction) and hemi-body pain (usually burning in nature and due to thalamic infarction) | |
Internal carotid | |
External carotid Hint: The internal carotid artery supplies blood to the brain. The external carotid artery supplies blood to the face and neck |
Question 2 |
Carotid Doppler ultrasound | |
Fundoscopic examination Hint: Important but may be normal in amaurosis fugax. | |
24-hour Holter monitor Hint: Useful if a cardiac source of emboli is suspected. | |
MRI of the brain Hint: Indicated if there are concerns for central nervous system pathology. | |
Fluorescein angiography Hint: Used for retinal vessel evaluation but not typically first-line in amaurosis fugax. |
Question 3 |
Immediate carotid endarterectomy Hint: Considered in cases with severe carotid stenosis and recurrent symptoms. | |
Antiplatelet therapy | |
Intravitreal injection of anti-VEGF agents Hint: Not indicated in amaurosis fugax. | |
Systemic corticosteroids Hint: Not effective in preventing amaurosis fugax. | |
Lifestyle modifications only Hint: Important but should be combined with medical therapy in the presence of significant carotid stenosis. |
|
List |
References: Merck Manual · UpToDate