Patient will present as → a 6-year old female who is being seen for a routine well-child exam is noted to have multiple teardrop-shaped growths partially obstructing the nasal passages. The child has a history of chronic sinusitis and recurring ear infections. As an astute PA, you order a sweat chloride test.
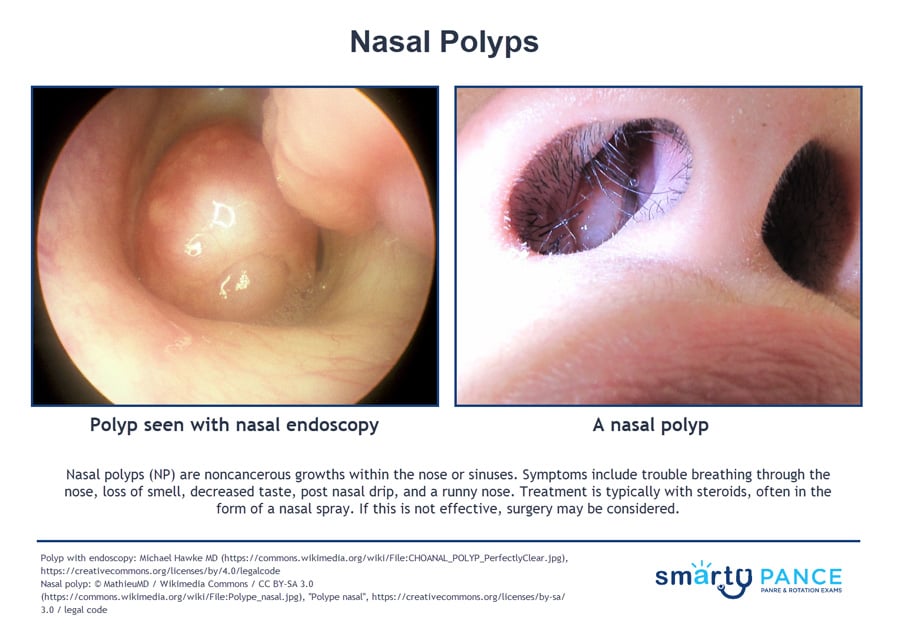
Nasal polyps (NP) are noncancerous growths within the nose or sinuses that appear as pale, boggy masses on the nasal mucosa
- Symptoms include trouble breathing through the nose, loss of smell, decreased taste, postnasal drip, and a runny nose
- Allergic rhinitis, acute and chronic infections, and cystic fibrosis all predispose to the formation of nasal polyps
- Finding nasal polyposis in a child is a “red flag” condition and should make the clinician suspicious of possible cystic fibrosis
- Samter's Triad is a chronic condition defined by asthma, sinus inflammation with recurring nasal polyps, and aspirin sensitivity
- It's also called aspirin-exacerbated respiratory disease (AERD), or ASA triad
Diagnosis is clinical
- Patients may complain of chronic congestion and a decreased sense of smell
A 3-month course of topical nasal corticosteroid is the initial treatment choice. This is effective for small polyps and can reduce the need for surgical intervention
- Oral steroids (6-day taper) can also help reduce the size
- Surgical removal may be necessary if therapy is unsuccessful or if polyps are large
Flashcards ready when you areYou have opened several Quizlet sets recently. Loading this one only when needed helps prevent a temporary Quizlet limit.
Question 1 |
Nasal polyps in a 3-year-old child should raise suspicion for which of the following conditions?
Allergic rhinitis Hint: While allergies are a major cause of nasal polyps in adults, they're far less likely to be the primary cause in young children. | |
Cystic fibrosis | |
Common cold Hint: Nasal congestion is a symptom of the common cold, but the development of true polyps is very atypical. | |
Samter's Triad Hint: Samter's Triad involves nasal polyps, asthma, and aspirin sensitivity. While important to recognize, it typically manifests in older patients. | |
Septal deviation Hint: Nasal polyps and septal deviation can both cause nasal obstruction. However, septal deviation would not explain the development of polyps, especially in a young child. |
Question 1 Explanation:
Nasal polyps, while relatively common in adults, are much less frequent in young children. Their presence in a child should prompt consideration of cystic fibrosis (CF), an inherited condition affecting the function of exocrine glands. Early diagnosis and treatment of CF are crucial.
Question 2 |
A 35-year-old man with a history of asthma and seasonal allergies presents with worsening nasal congestion and a decreased sense of smell for the past several months. He has had recurrent sinus infections throughout the year. Examination reveals pale, smooth, grape-like masses obstructing both nasal passages. Which of the following is the most appropriate initial management for this patient?
Amoxicillin Hint: While antibiotics are appropriate for treating recurrent sinus infections, they are not the initial treatment for nasal polyps themselves. | |
Desloratadine Hint: Antihistamines, like desloratadine, can be helpful in managing nasal allergy symptoms, but they don't target the underlying inflammation of nasal polyps. | |
Fluticasone nasal spray | |
Prednisone taper Hint: Systemic corticosteroids, like prednisone, can help shrink polyps in the short term, but they come with a risk of significant side effects, making them less desirable for initial management. They may be utilized for short-term symptom control in severe cases. | |
Sinuplasty Hint: Sinuplasty involves procedures to open the sinus passages. While surgery might be indicated for chronic, recurrent polyps that don't respond to medical therapy, it is not an initial treatment. |
Question 2 Explanation:
The patient's clinical presentation is consistent with nasal polyps. Intranasal corticosteroids, like fluticasone nasal spray, are the cornerstone of medical therapy for nasal polyps. They reduce inflammation and help manage the underlying allergic disease process.
Question 3 |
A 45-year-old woman with a history of aspirin sensitivity, asthma, and chronic sinusitis presents with persistent nasal obstruction and facial pressure. She has frequent exacerbations of her asthma despite using inhaled corticosteroids and a long-acting beta-agonist. Nasal endoscopy reveals bilateral polypoid masses. In addition to optimizing her asthma management, which of the following is the most appropriate next step for this patient?
Computed tomography (CT) scan of the sinuses Hint: While a CT scan is often obtained to visualize sinus anatomy in chronic sinusitis patients, it does not address the patient's underlying aspirin sensitivity, which is a major aspect of this case. | |
Desensitization therapy to aspirin | |
Montelukast Hint: Montelukast, a leukotriene inhibitor, can be helpful in general asthma management, but its role in Samter's Triad is less substantial compared to aspirin desensitization. | |
Omalizumab Hint: This biologic medication targets IgE and can be a valuable treatment for severe allergic asthma, but it does not directly address the aspirin sensitivity component of this case. | |
Septoplasty Hint: A septoplasty is a surgical procedure that corrects a deviated septum. While it might be indicated in some cases of nasal obstruction, it does not address the underlying inflammation and aspirin sensitivity of Samter's Triad. |
Question 3 Explanation:
This patient presents with Samter's Triad, a condition characterized by nasal polyps, asthma, and aspirin sensitivity. Aspirin desensitization therapy, followed by continued daily aspirin, can greatly improve both chronic sinusitis symptoms and asthma control in these patients.
There are 3 questions to complete.
|
List |
References: Merck Manual · UpToDate