Nose and Sinus Disorders (PEARLS)
NCCPA™ PANCE EENT Content Blueprint ⇒ nose and sinus disorders
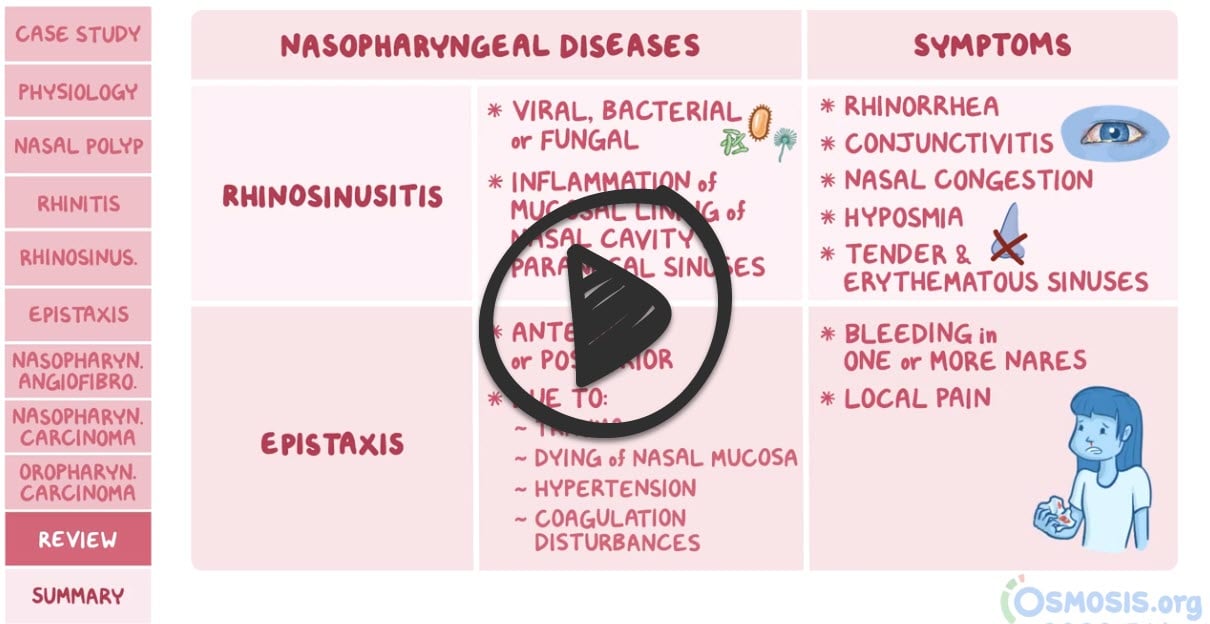
 Osmosis (High Yield Nasopharyngeal Diseases) Osmosis (High Yield Nasopharyngeal Diseases) |
 |
| Epistaxis (ReelDx) |
Epistaxis
 You are called to see a 9-year-old with acute onset epistaxis and low platelet count You are called to see a 9-year-old with acute onset epistaxis and low platelet count
Patient
- Gender: Male
- Age: 9 years
Vitals
- Temperature: Not Available
- Blood Pressure: 97/66
- Heart Rate: 98
- Respiratory Rate: 20
- Pulse Oximetry: 100% RA
Signs and Symptoms
Click here to work through this patient case simulation.
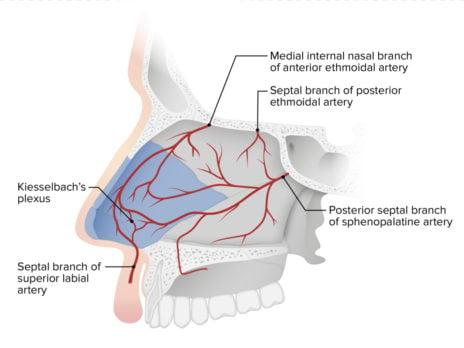
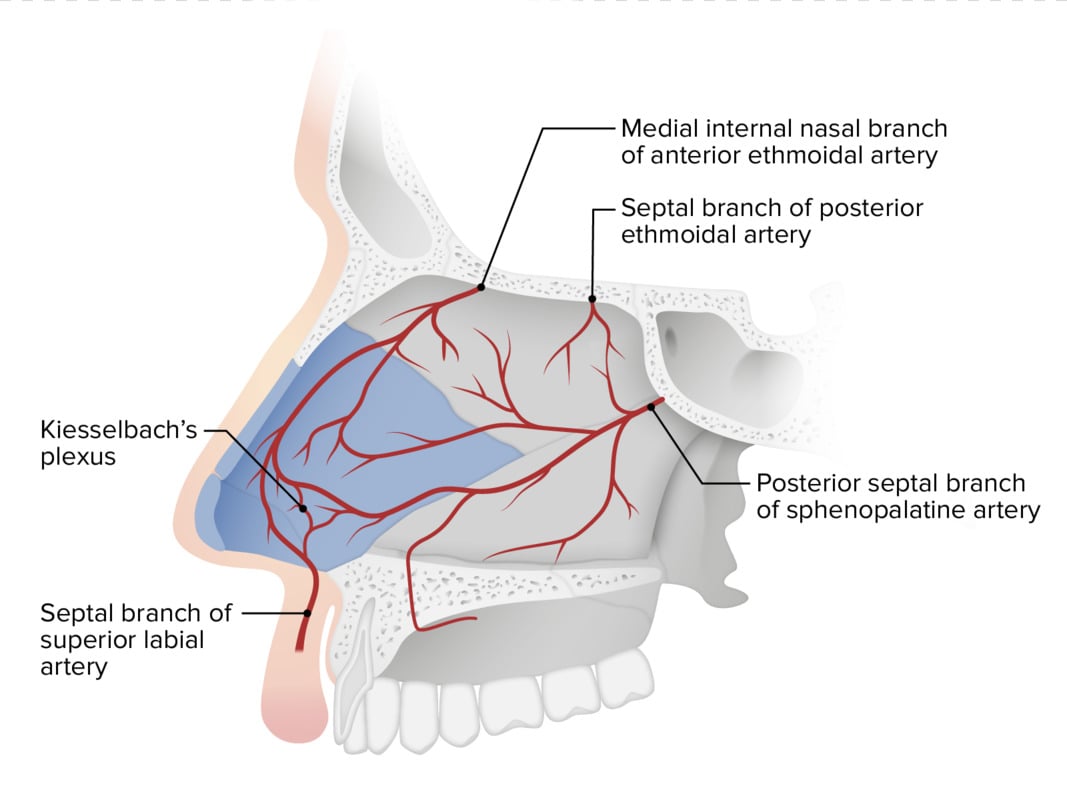
Patient will present as → a 14-year-old who is brought to your Emergency Department (ED) with an intractable nosebleed. Pinching of the nose has failed to stop the bleeding. In the ED, a topical vasoconstrictor is tried but also fails to stop the bleeding. Kiesselbach's Plexus or Little's Area is the most common site for anterior bleeds
The sphenopalatine artery (Woodruff’s plexus) is generally the source of severe posterior nosebleeds. Direct pressure for 15 minutes, posterior balloon packing is used to treat posterior epistaxis
DX: The majority do not require testing other than direct visualization
- Patients with symptoms or signs of a bleeding disorder and those with severe or recurrent epistaxis should have CBC, PT, and PTT.
- CT may be done if a foreign body, a tumor, or sinusitis is suspected.
TX: Most nosebleeds are anterior and stop with direct pressure
- Apply direct pressure for at least 10-15 minutes, seated and leaning forward
- Short-acting topical decongestants (Afrin, phenylephrine, cocaine)
- Anterior nasal packing
- Patients with nasal packing must be treated with antibiotics (cephalosporin) to prevent toxic shock syndrome, and the patient has to return to take the packing out.
- If there is no packing in the nose, place a small amount of petroleum jelly or antibiotic ointment inside the nostril 2 times a day for 4–5 days
- Posterior balloon packing is used to treat posterior epistaxis. These patients must be admitted to the hospital, and prompt consultation with an otolaryngologist is indicated
- Recurrent epistaxis: Must rule out hypertension or coagulation disorder (like vWD)
|
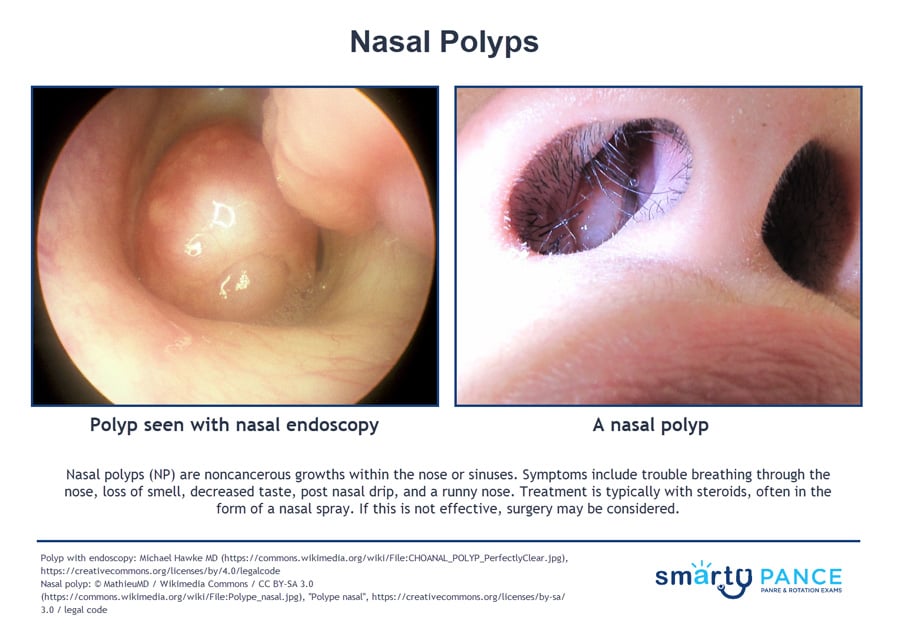
| Nasal polyps |
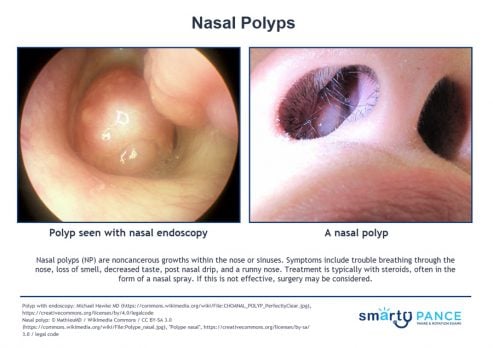
Patient will present as → a 42-year-old man with a history of severe asthma and aspirin intolerance presents with bilateral nasal obstruction, anosmia (loss of smell), and chronic post-nasal drip for over 2 years. Anterior rhinoscopy reveals pale, glistening grape-like masses protruding from both middle meatuses. CT sinuses shows bilateral opacification of ethmoid sinuses with polypoid masses. Teardrop-shaped growths that form in the nose or sinuses
- Samter's triad:
- asthma
- aspirin sensitivity
- nasal polyps
- Usually benign, often with allergic rhinitis. Consider Cystic Fibrosis when multiple polyps are seen
- Chronic congestion and decreased sense of smell
DX: Diagnosis is clinical
- Patients may complain of chronic congestion and a decreased sense of smell
TX: Topical nasal corticosteroid (3-month course) is the initial treatment choice. This is effective for small polyps and can reduce the need for surgical intervention.
- Oral steroids (6-day taper) can also help reduce the size
- Surgical removal may be necessary if therapy is unsuccessful or if polyps are large
|
| Rhinitis (ReelDx) |
Rhinitis
 You are called to see a 6-year-old girl with increasing bilateral nosebleeds over the past week You are called to see a 6-year-old girl with increasing bilateral nosebleeds over the past week
Patient
- Gender: Female
- Age: 6 years
- Weight: 54 lb/24.5 kg
- Height: 48.3 in/122.7 cm
Vitals
- Temperature: 98.1 F/36.7 C
- Heart Rate: 81
- Respiratory Rate: 20
- Pulse Oximetry: 100% RA
Signs and Symptoms
- Increasing bilateral nosebleeds over the past week; otherwise, well
Click here to work through this patient case simulation.
Patient will present as → a 13-year-old boy with clear fluid discharge from his nose for 2 days duration. This has also been associated with sneezing. On nasal exam, the mucosa and turbinates appear edematous and slightly bluish. He has swollen dark circles under his eyes and a transverse nasal crease. Rhinitis is inflammation of the nasal mucosa characterized by sneezing, nasal congestion, runny nose (rhinorrhea), and postnasal drip
- Types include:
- Allergic rhinitis (IgE-mediated mast cell histamine release, seasonal or perennial)
- Viral (infectious) rhinitis (common cold)
- Nonallergic rhinitis (vasomotor, hormonal, medication-induced)
- Allergic rhinitis presents with sneezing, clear rhinorrhea, nasal congestion, itchy eyes/nose, allergic shiners, and often atopic comorbidities (e.g., asthma, eczema)
- Physical exam may reveal pale, boggy nasal turbinates, allergic shiners, and a transverse nasal crease
DX: Diagnosis is clinical; skin testing or serum IgE testing may help confirm allergen sensitivities
TX: Avoid any known allergens and use antihistamines, cromolyn sodium, nasal or systemic corticosteroids, nasal saline drops or washes, and immunotherapy
- Intranasal corticosteroids (first-line for allergic rhinitis)
- Antihistamines (oral or intranasal)
- Decongestants (short-term use only)
- Intranasal decongestants (e.g. Afrin) should not be used for more than 3-5 days, as they may cause rhinitis medicamentosa
- Allergen avoidance and immunotherapy in selected cases
- Nonallergic rhinitis may be triggered by temperature changes, strong odors, medications, or hormonal shifts
- Vasomotor rhinitis responds well to intranasal iproptrium bromide
- Complications include sinusitis, sleep disturbance, and impaired quality of life
 Allergic shiners
 Allergic salute with transverse nasal crease |
| Sinusitis (ReelDx) |
Sinusitis

24 y/o with fever and right-sided sinus pain
Patient
- Gender: Female
- Age: 24
- Weight: 218 lb / 99 kg
- Height: 64 in / 162 cm
Vitals
- Temperature: 98.3 F/36.8 C
- Blood Pressure: 143/61 mmHg
- Heart Rate: 61
- Respiratory Rate: 18
- Pulse Oximetry: 94% RA
Signs and Symptoms
Cough; fever; right-sided sinus pain, especially upon Palpation, headache, ear pain that is itchy, Vomiting; the patient’s symptoms began yesterday
Click here to work through this patient case simulation.
Patient will present as → a 34-year-old previously healthy male with complaints of facial pressure and rhinorrhea for the past 3 weeks. The patient reports that several weeks prior, he had a “common cold,” which resolved. However, he has since developed worsening facial pressure, especially over his cheeks and forehead. He reports over 1 week of green-tinged rhinorrhea. His temperature is 100.1 F (37.8 C), blood pressure is 120/70 mmHg, pulse is 85/min, and respirations are 15/min. The nasal exam reveals edematous turbinates and purulent discharge. The patient has facial tenderness with palpation over the involved sinus. After URI. Sinus pain/pressure (worse with bending down and leaning forward). Facial tap elicits pain.
- Viral: Most common, symptoms < 7 days. Bacterial: Symptoms 7+ days and associated with bilateral purulent nasal discharge
- Organisms: S. pneumoniae, H. influenzae, M.catarhalis
- Chronic = lasts 12 weeks or longer
DX: Plainview X-ray (water's view) is a good initial screening; CT is the Gold Standard
TX: Indications for antibiotics in rhinosinusitis include the duration of symptoms >10 days without improvement, onset of fever > 102.2, and purulent nasal discharge or facial pain > 3-4 days, and worsening of symptoms after viral URI > 5-6 days that was initially improving
- Amoxicillin-clavulanate 875 mg/125 mg orally twice daily (x 7 days adults and 14 days pediatrics)
- Penicillin-allergic: Doxycycline 100 mg orally twice daily (x 7 days adults and 14 days pediatrics)
**Macrolides (clarithromycin or azithromycin) and trimethoprim-sulfamethoxazole are not recommended for empiric therapy because of high rates of resistance to S. pneumoniae
Risk for resistance or antibiotic failure
- Augmentin 2 g PO BID (x 7 days adults and 14 days pediatrics)
- Levofloxacin 750 mg PO daily once daily x 7 days
Chronic rhinosinusitis (CRS) lasts 12 weeks or longer despite attempts at medical management. Therapy is typically given for at least three weeks and may be extended for up to ten weeks in refractory cases
- Amoxicillin-clavulanate: 875 mg twice daily or two 1000 mg extended-release tablets twice daily
- Pen allergic: Clindamycin 300 mg four times daily or 450 mg three times daily
 Front view illustration and side-by-side CT scans of normal and chronic sinusitis |
| Trauma and Nasal foreign body (ReelDx) |
Nasal foreign body

4 y/o with foul odor from the nose for 2 weeks
Patient
- Gender: Male
- Age: 4Signs and Symptoms
- Foul odor from the nose for 2 weeks
Click here to work through this patient case simulation.
Patient will present as → a 4-year-old boy with unilateral purulent, foul-smelling nasal discharge for three days. The child has no other respiratory symptoms. Unilateral foul-smelling purulent nasal discharge — hallmark; often misdiagnosed as sinusitis
- Persistent foul-smelling purulent unilateral nasal discharge in a young child without other respiratory symptoms should raise suspicion for a retained nasal foreign body, even without a history of witnessed foreign body insertion.
DX: Diagnosis is clinical
TX: Prior to removal, consider using oxymetazoline drops to shrink the mucous membrane |
Back to PANCE Blueprint EENT (6%)


.jpg)
{kind=link}
{kind=link}
{kind=link}