 Lecture
LecturePatient will present as → a 30-year-old female presents with gradual hearing loss in her right ear over the past year, now affecting her left ear. She struggles to hear low-pitched sounds and conversations in noisy settings. Examination shows conductive hearing loss with normal otoscopic findings. Audiometry confirms bilateral conductive hearing loss and tympanometry shows reduced compliance. A CT scan confirms the diagnosis of otosclerosis. Treatment options include hearing aids and surgical interventions such as stapedectomy or stapedotomy. She is referred to an otolaryngologist for further evaluation and advised on the benefits and risks of surgery and the importance of regular follow-up.

To watch this and all of Joe Gilboy PA-C's video lessons you must be a member. Members can log in here or join now.
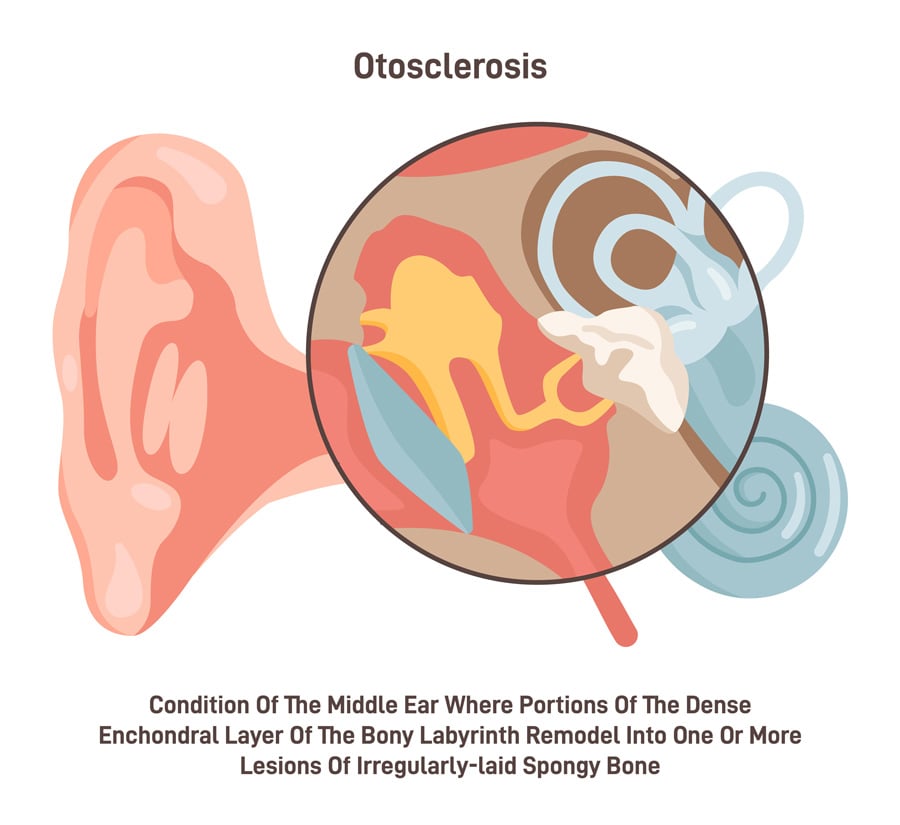
Otosclerosis is a bony overgrowth that involves the footplate of the stapes, causing conductive hearing loss. It is a leading cause of conductive hearing loss in adults
- The stapes can no longer function as a piston, gradually becoming fixated, leading to hearing loss up to 60 dB
- Symptoms include gradual hearing loss, especially in the low-frequency range, and tinnitus (+/- vertigo)
- More common in females and typically presents in young adults
- Autosomal dominant inheritance with variable penetrance
- Positive family history in many cases - There is a 25% chance of developing otosclerosis if one parent has it and a 50% chance if both parents have it
- Typically, otosclerosis develops in one ear, although more than half of patients continue developing symptoms in both ears
- The Weber test may lateralize to the affected ear, and the Rinne test will show bone conduction greater than air conduction in the affected ear
© inspiring.team / Adobe Stock
Otosclerosis vs. Presbycusis (age-related hearing loss)
While otosclerosis and presbycusis can both cause hearing loss, there are key differences:
- Otosclerosis typically causes conductive hearing loss, while presbycusis causes sensorineural hearing loss.
- Otosclerosis often presents in young to middle-aged adults, while presbycusis is associated with age-related changes in the inner ear.
- Otosclerosis may have a family history and can be associated with tinnitus +/- vertigo, while presbycusis is not typically associated with these symptoms.
- The hearing loss in otosclerosis can be treated with surgery or hearing aids, while presbycusis is managed primarily with hearing aids.
Diagnosed with audiometry (audiogram), showing conductive hearing loss. CT scan can confirm the diagnosis by showing bone changes
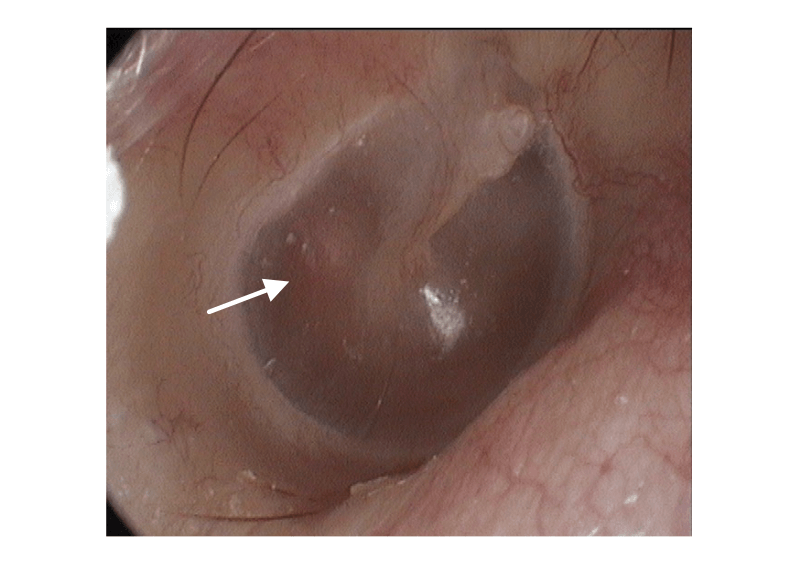
- Otoscopic examination is usually normal, although in some cases, a reddish hue (Schwartze sign) may be seen over the promontory
- Tympanometry may show a normal or reduced compliance
- Differential diagnosis includes chronic otitis media, cholesteatoma, and ossicular chain discontinuity
{kind=link}
Treatment involves either hearing amplification or surgical intervention
- Hearing aids can be beneficial in the early stages
- Surgical options include stapedectomy (involves creating a small hole in the footplate of the stapes) or stapedotomy where the stapes is replaced with a prosthesis
- In advanced cases, cochlear implantation may be considered
- Oral sodium fluoride therapy (a common treatment in France) is not routinely recommended in the US due to limited efficacy and potential side effects
Question 1 |
Accumulation of cerumen in the ear canal Hint: While cerumen impaction can cause conductive hearing loss, it is typically detected via otoscopic examination and is not associated with familial patterns or gradual worsening over years. | |
Degeneration of the cochlear hair cells Hint: This mechanism is associated with sensorineural hearing loss, commonly seen in presbycusis or noise-induced hearing loss, not with the conductive hearing loss seen in otosclerosis. | |
Fixation of the stapes bone in the middle ear | |
Eustachian tube dysfunction Hint: This can cause conductive hearing loss due to middle ear effusion but does not involve stapes fixation or familial predisposition. | |
Sensorineural damage due to autoimmune disease Hint: Autoimmune inner ear disease causes sensorineural, not conductive, hearing loss and typically presents with rapid onset and systemic autoimmune symptoms. |
Question 2 |
CT scan of the temporal bone | |
Magnetic resonance imaging (MRI) Hint: MRI is less effective than CT in visualizing bony changes specific to otosclerosis. | |
Brainstem auditory evoked response (BAER) Hint: BAER is used to evaluate the auditory pathway up to the brainstem and is not specific for diagnosing otosclerosis. | |
Pure tone audiometry Hint: While audiometry can suggest conductive hearing loss, it cannot definitively diagnose otosclerosis. | |
Rinne and Weber tests Hint: These tests can help differentiate between conductive and sensorineural hearing loss but cannot confirm otosclerosis. |
Question 3 |
Cochlear implant Hint: This is used for severe to profound sensorineural hearing loss and is not appropriate for conductive hearing loss due to otosclerosis. | |
Hearing aids | |
Oral corticosteroids Hint: These are not effective for otosclerosis as it is a bony abnormality, not an inflammatory condition. | |
Antibiotic therapy Hint: Antibiotics are not indicated in otosclerosis, as it is not an infectious process. | |
Tympanostomy tube insertion Hint: Tubes are used for middle ear effusion and Eustachian tube dysfunction, not for otosclerosis. |
|
List |
References: Merck Manual · UpToDate