NCCPA™ PANCE EENT Content Blueprint eye disorders ⇒ vision abnormalities
The "Curtain Coming Down" Clinical Comparison: Amaurosis Fugax vs. Retinal Detachment
| Feature | Amaurosis Fugax | Retinal Detachment |
| "Curtain" Presentation | Transient "Curtain": Vision loss is temporary (seconds to minutes) and then completely resolves. | Persistent "Curtain": Vision loss is fixed and may expand over time as the retina continues to peel. |
| Pathophysiology | Vascular Ischemia: An embolus (often from the carotid) briefly blocks retinal blood flow. | Mechanical Separation: The retina physically detaches from the choroid layer. |
| Warning Signs | Usually none, but may have a history of previous TIAs or carotid bruits. | Flashes (photopsia) and a sudden shower of floaters often precede the curtain. |
| Fundoscopic Findings | Often normal, but may show a Hollenhorst plaque (glistening yellow cholesterol embolus). | Retina appears grey and wrinkled; may look like a "billowing sail" or cloud. |
| Most Likely Next Step | Carotid Ultrasound and EKG to find the source of the clot. | Emergent Ophtho Consultation for surgical reattachment. |
| Risk Factors | Hypertension, smoking, and carotid artery stenosis. | High myopia (nearsightedness), trauma, or eye surgery. |
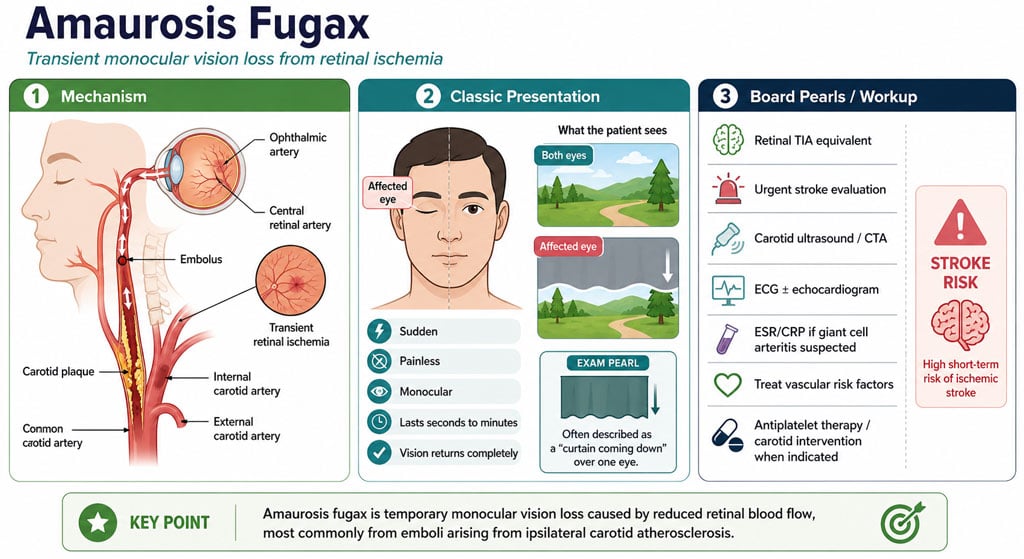
| Amaurosis fugax | Patient will present as → an 82-year-old man who presents to the emergency department complaining of vision loss in his left eye. He states that it suddenly appeared as if a curtain was coming down over his left eye. It resolved after five minutes, and his vision has returned to normal. He has a history of coronary artery disease and type 2 diabetes.
Amaurosis fugax (amaurosis meaning darkening, dark, or obscure, fugax meaning fleeting) is a painless temporary loss of vision in one or both eyes
Five distinct classes based on their supposed cause: embolic, hemodynamic, ocular, neurologic, and idiopathic
DX: A fundus exam may reveal optic disk pallor, a cherry-red macula (retinal vascular occlusion), and retinal edema
TX: If the diagnostic workup reveals a systemic disease process, directed therapies to treat that underlying cause should be initiated
|
| Amblyopia | Patient will present as → a 5-year-old male is brought by his parents and referred by his teacher for suspected decreased vision in his left eye. His mother had not noticed any vision problems. He has had normal growth and development. On exam, the patient has an abnormal vision screen of the left eye and red reflex asymmetry. Amblyopia (lazy eye) is reduced visual acuity that is not correctable by refractive means
DX: screening to detect amblyopia in all children younger than five years of age
TX: Includes correction of refraction error as well as forced use of the amblyopic eye by patching the better eye or blurring with glasses or drops |
| Glaucoma | 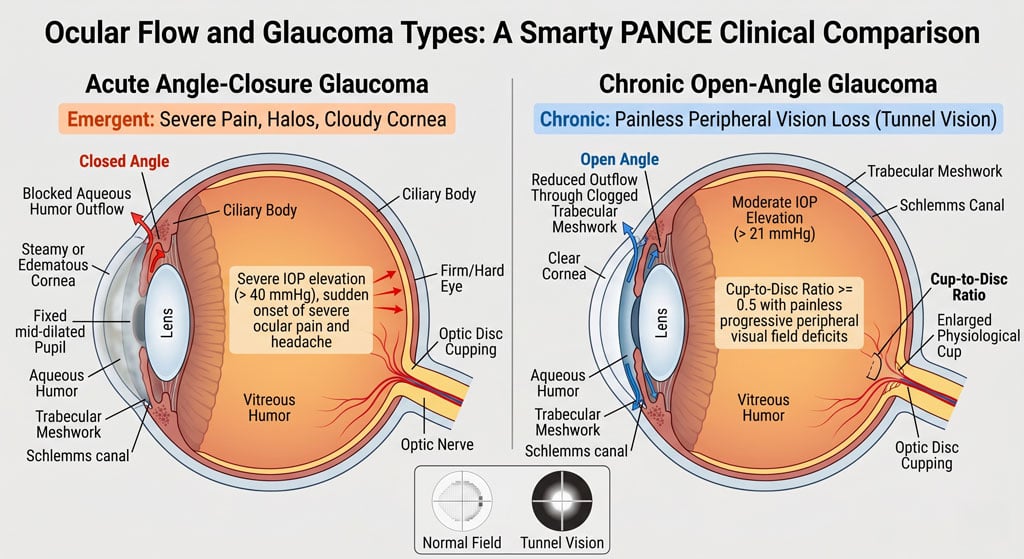
Patient with open-angle glaucoma present as → a 47-year-old African American male presents for an ophthalmic examination. Medical history is significant for hypertension and type II diabetes mellitus. On slit-lamp examination, there is cupping of the optic disc, with a cup-to-disc ratio > 0.6. Tonometry reveals intraocular pressure of 45 mmHg (normal is 8-21 mmHg). Peripheral field vision loss is noted on the visual field exam. Patient with acute angle-closure glaucoma will present with → a 60-year-old Asian American woman presents with sudden ocular pain. She reports she was visiting the planetarium when the pain started, and when she walked outside, she saw halos around the street lights. The pain was so bad that she began to vomit. She reports her vision is decreased. Physical examination reveals conjunctival injection, a cloudy cornea, and pupils Open-angle glaucoma: most common, aqueous outflow obstruction
Acute narrow angle-closure glaucoma: Iris against the lens, dark environment, acute loss of vision, nausea, and vomiting.
DX: Diagnosis is confirmed by tonometry demonstrating increased intraocular pressure
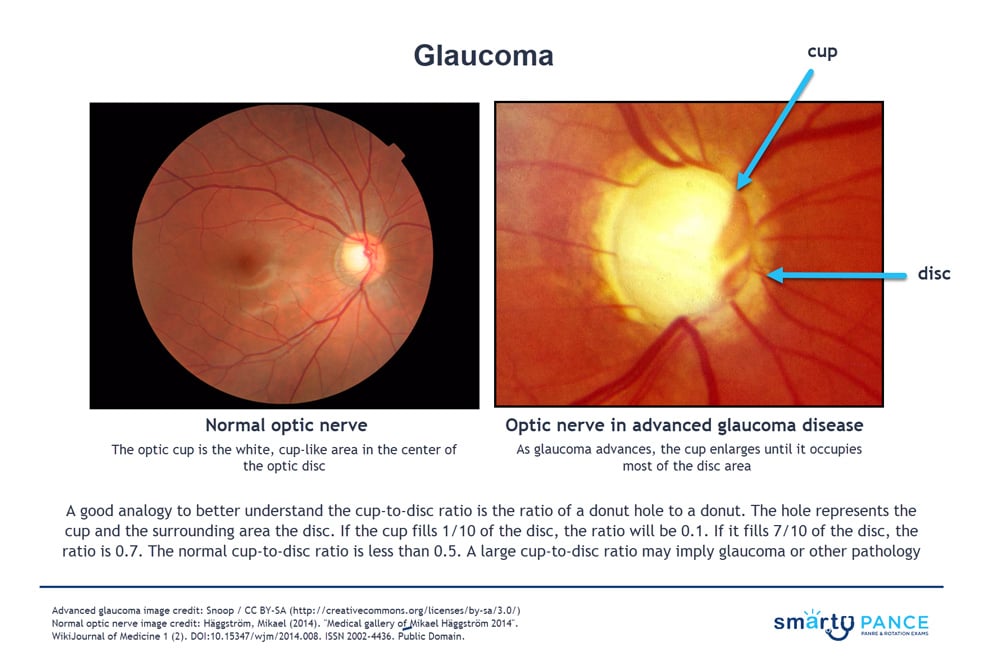
All patients should be screened at age 40 - may present for routine fundoscopy with a cup-to-disk ratio > 0.5 (<0.5 is normal). This is suggestive but not diagnostic of glaucoma, so you will progress to the next step, which is tonometry
TX: Acute narrow angle-closure glaucoma
Chronic open-angle glaucoma
|
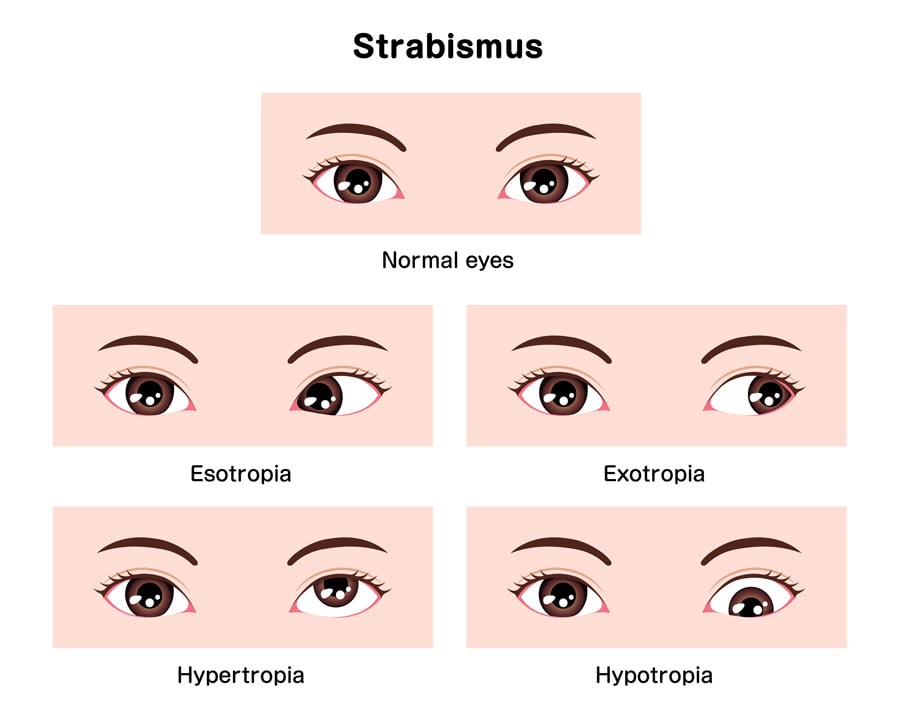
| Strabismus (ReelDx) | ReelDx Virtual Rounds (Strabismus )Patient will present as → a 3-year-old girl brought to you by her mother, who is worried about her daughter’s “lazy eye.”She reports that her daughter’s symptoms are exaggerated when she has a cold. Past medical history is negative for trauma or headaches. The patient has an asymmetric corneal light reflex, and the cover/uncover test reveals a right-sided esotropia. You refer the patient to a pediatric ophthalmologist. Strabismus is defined as any form of ocular misalignment
DX: The cover/uncover test is used to diagnose strabismus
TX: Treatment options can include glasses, occlusion therapy, orthoptic exercises, surgery, or a combination of these therapies
|
| Presbyopia | Patient will present as → a 45-year-old female, accountant, presents with complaints of difficulty reading small print and needing to hold reading materials farther away to see clearly. She mentions headaches and eye strain after prolonged reading or computer use. These symptoms started gradually over the past year and have become more bothersome. She denies any significant changes in vision aside from these near-vision difficulties. Presbyopia is an age-related condition causing gradual loss of the eye's ability to focus on nearby objects, typically starting in the early to mid-40s and affecting nearly everyone by age 65
DX: Diagnosis involves a comprehensive eye exam with visual acuity tests, refraction assessments, near vision tests, and slit-lamp examinations. TX: Treatment options focus on improving near vision and include eyeglasses, contact lenses, refractive surgery, lens implants, and lifestyle modifications such as using good lighting and taking breaks during prolonged near work |

{kind=link}