Other abnormalities of the ear (PEARLS)
NCCPA™ PANCE EENT Content Blueprint ⇒ ear disorders ⇒ other abnormalities of the ear
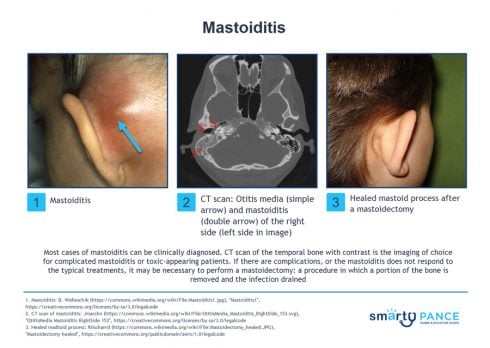
| Mastoiditis (ReelDx) |
Mastoiditis
 You are called to see a 10 y/o with ear pain worsening over the last 5 days You are called to see a 10 y/o with ear pain worsening over the last 5 days
Patient
- Gender: Male
- Age: 10 years
- Weight: 81 lb/36.7 kg
- Height: 56 in/142.2 cm
Vitals
Signs and Symptoms
- Otalgia, worsening over the last 5 days; nasal congestion; afebrile
Click here to work through this patient case simulation.
Patient will present as → a 10-year-old boy with otalgia, worsening over the last 5 days and associated with nasal congestion. The patient is afebrile with a temperature of 98 ° F. Examination reveals edema of the external auditory canal, producing an anterior and inferior displacement of the auricle with percussion tenderness posteriorly. Suppurative infection of mastoid air cell ⇒ usually a complication of acute otitis media
- Presents with fever, otalgia, pain & erythema posterior to the ear, and forward displacement of the external ear
- Organisms: S. pneumoniae, H. influenzae, M. catarrhalis, S. aureus, S. pyogenes
DX: Clinical; CT scan temporal bone with contrast for complicated/toxic appearing
TX: IV antibiotics + drainage are the mainstay of treatment
- First-line (no recent antibiotics): Ampicillin–sulbactam IV (covers S. pneumoniae, S. pyogenes)
- If recent antibiotics or recurrent AOM: Piperacillin–tazobactam IV (adds Pseudomonas coverage)
- Add vancomycin if severe illness, sepsis, or concern for MRSA
- IV therapy for 7–10 days, then oral antibiotics to complete ~4 weeks total
Procedures
- Myringotomy ± tympanostomy tube for middle ear drainage
- Simple mastoidectomy (drains abscess, removes infected mastoid cells) if no improvement within 48 hrs or if abscess forms
|
| Meniere disease |
Patient will present as → a 45-year-old woman presents with recurrent episodes of severe episodic rotational vertigo lasting 2–4 hours, associated with fluctuating left-sided hearing loss, low-pitched tinnitus, and a sensation of aural fullness in the left ear. The episodes are preceded by a feeling of pressure in the ear. She has had 5 similar episodes over the past year. Between attacks, she has mild residual hearing loss on the left. Ménière syndrome is a disorder of the endolymphatic compartment with the classic triad of episodic vertigo, unilateral low-frequency sensorineural hearing loss, and tinnitus.
"Meniere's disease is associated with EPISODIC vertigo and NOT associated with viral infections. This differentiates it from Labyrinthitis, which is associated with CONTINUOUS vertigo along with hearing loss +/- tinnitus and is usually associated with an upper respiratory infection."
DX: Clinical diagnosis (AAO-HNS criteria): ≥2 definitive vertigo episodes (20 min–24 h) + audiometrically documented SNHL + ipsilateral tinnitus or aural fullness + no other diagnosis
- Although audiometric testing is a required part of the diagnostic evaluation, there is no specific diagnostic test for MD
- Imaging (MRI with gadolinium enhancement), although not required for the diagnosis of MD, is frequently performed to exclude important disorders that can present with similar symptoms.
A clinical diagnosis of MD is made based on the following criteria:
- Two or more spontaneous episodes of vertigo, each lasting 20 minutes to 12 hours
- Audiometrically documented low- to mid-frequency sensorineural hearing loss in the affected ear
- Fluctuating aural symptoms (reduced or distorted hearing, tinnitus, or fullness) in the affected ear
- Symptoms not better accounted for by another vestibular diagnosis
TX: Lifestyle modifications (first-line): low-sodium diet (<1,500–2,000 mg/day), reduce caffeine, alcohol, stress
- Diuretics: hydrochlorothiazide/triamterene or acetazolamide — reduce endolymph production
- Betahistine: improves cochlear blood flow; widely used in Europe (limited FDA approval)
- Acute attack: vestibular suppressants (meclizine, diazepam), antiemetics
- Intratympanic gentamicin: ablates vestibular function in refractory cases; preserves hearing better than surgical approaches
- Intratympanic steroids: for acute hearing loss episodes; less effective for vertigo
- Endolymphatic sac surgery or labyrinthectomy/vestibular neurectomy: for medically refractory severe cases
|
| Tinnitus |
Patient will present as → a 70-year-old female who states that her children and grandchildren have asked her to seek medical attention as she seems to be losing her hearing. She also describes an occasional ringing, buzzing, and hissing sound. She is in generally good health, and her only medications are a multivitamin along with calcium and vitamin D. You examine her ears and find the external auditory canals to be free of cerumen and the tympanic membranes to be normal in appearance. A perceived sensation of sound in the absence of an external acoustic stimulus is often described as ringing, hissing, buzzing, or whooshing.
- 90% are associated with sensorineural hearing loss – caused by loud noise, presbycusis, medications (aspirin, antibiotics, aminoglycosides, loop diuretics, and CCBs), Meniere's disease, acoustic neuroma, TMJ disorders, AVMs, and atherosclerosis
DX: All patients with significant tinnitus should be referred for comprehensive audiologic evaluation to determine the presence, degree, and type of hearing loss.
- In patients with unilateral tinnitus+ hearing loss, acoustic neuroma should be ruled out by gadolinium-enhanced MRI
- In patients with unilateral tinnitus and normal hearing and physical examination, MRI is not necessary unless tinnitus persists > 6 mo.
TX: No pharmacologic agent has been shown to cure or consistently alleviate tinnitus
- The goal is to try to identify the cause, i.e., remove ototoxic medications
- Hearing aids for tinnitus with hearing loss
- CBT or sound therapy (white noise machines) for persistent, bothersome tinnitus
- Medications (TCAs such as amitriptyline and nortriptyline)
- Alternative therapies include acupuncture, hypnosis, melatonin
|
Back to PANCE Blueprint EENT (6%)

