 Picmonic
Picmonic

56 y/o with intermittent loss of vision in the right eye
Patient will present as → a 57-year-old male with a history of hypertension who complains of an acute onset of intermittent headaches and blurred vision of the right eye.
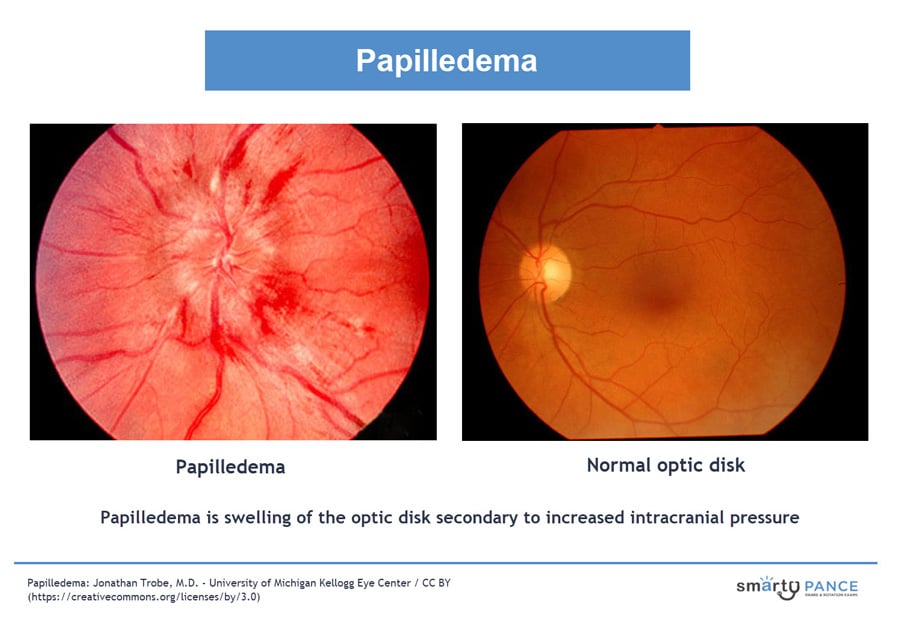
Papilledema is swelling of the optic disk secondary to increased intracranial pressure → classically bilateral but (as in the video example) may be unilateral
- Optic disk swelling resulting from causes that do not involve increased intracranial pressure (eg, malignant hypertension, thrombosis of the central retinal vein) is not considered papilledema.
- There are no early symptoms, although vision may be disturbed for a few seconds. Papilledema requires an immediate search for the cause
Diagnosis is by ophthalmoscopy with further tests, usually brain imaging and sometimes subsequent lumbar puncture, to determine the cause
- MRI or CT scan of the head looking for a cause. Focus on finding intracranial pathology = tumor or bleed, cerebral edema, CSF outflow obstruction or overproduction
- Increased opening pressure with lumbar puncture confirms increased intracranial pressure
Causes include the following:
- Brain tumor or abscess
- Cerebral trauma or hemorrhage
- Meningitis
- Arachnoidal adhesions
- Cavernous or dural sinus thrombosis
- Encephalitis
- Idiopathic intracranial hypertension (pseudotumor cerebri), a condition with elevated CSF pressure and no mass lesion
Urgent treatment of the underlying disorder is indicated to decrease intracranial pressure.
- If intracranial pressure is not reduced, secondary optic nerve atrophy and vision loss eventually occur, along with other serious neurologic sequelae.
 Intracranial pressure (ICP) is a measure of the hydrostatic pressure in the brain. Three elements contribute to ICP: brain tissue, blood, and cerebrospinal fluid (CSF). While these elements usually remain in balance, factors such as an increased body temperature or increased arterial or venous pressures can cause the ICP to fluctuate. The Monro-Kellie doctrine states, that if one component of ICP (brain tissue, blood, CSF) increases, one of the other components will decrease to maintain a constant pressure. When this balance is disrupted or when compensatory mechanisms fail, increased ICP can result. Signs and symptoms of increased ICP include a change in the level of consciousness, headache, irregular respirations, widening pulse pressure, bradycardia, projectile vomiting, abnormal pupils, and decerebrate or decorticate posturing.
Intracranial pressure (ICP) is a measure of the hydrostatic pressure in the brain. Three elements contribute to ICP: brain tissue, blood, and cerebrospinal fluid (CSF). While these elements usually remain in balance, factors such as an increased body temperature or increased arterial or venous pressures can cause the ICP to fluctuate. The Monro-Kellie doctrine states, that if one component of ICP (brain tissue, blood, CSF) increases, one of the other components will decrease to maintain a constant pressure. When this balance is disrupted or when compensatory mechanisms fail, increased ICP can result. Signs and symptoms of increased ICP include a change in the level of consciousness, headache, irregular respirations, widening pulse pressure, bradycardia, projectile vomiting, abnormal pupils, and decerebrate or decorticate posturing.
| Increased Intracranial Pressure (ICP) Assessment | Play Video + Quiz |
| Increased Intracranial Pressure (ICP) Interventions | Play Video + Quiz |
Question 1 |
Acute angle-closure glaucoma Hint: Typically presents with painful, red eye and vision loss. | |
Diabetic retinopathy Hint: Causes microvascular changes in the retina, not optic disc swelling. | |
Increased intracranial pressure | |
Hypertensive retinopathy Hint: Characterized by retinal vascular changes, not typically optic disc swelling. | |
Central retinal vein occlusion Hint: Usually unilateral and presents with sudden vision loss. |
Question 2 |
Order a CT scan of the head Hint: This is typically performed to rule out intracranial pathology, but an MRI has already been done and is more sensitive. | |
Perform a lumbar puncture | |
Initiate therapy with high-dose prednisone Hint: Corticosteroids are not the first-line treatment for IIH and are typically reserved for cases with severe vision loss or other complications. | |
Conduct a stat cerebral arteriogram Hint: This would be indicated if there was suspicion of a vascular abnormality, which is not suggested by the current findings. | |
Provide reassurance and schedule a follow-up in 6 months Hint: Given the presence of papilledema and the potential risk for permanent vision loss, immediate action is required rather than mere reassurance and delayed follow-up. |
Question 3 |
Acetazolamide | |
Topical beta-blockers Hint: Used in the treatment of glaucoma, not indicated for IIH. | |
Surgical optic nerve sheath decompression Hint: Considered in cases with severe or progressive vision loss. | |
Systemic corticosteroids Hint: Not the first-line treatment for IIH. | |
Weight loss and lifestyle modification Hint: Important adjunctive measures, especially in overweight patients, but acetazolamide is the primary initial treatment. |
|
List |
References: Merck Manual · UpToDate