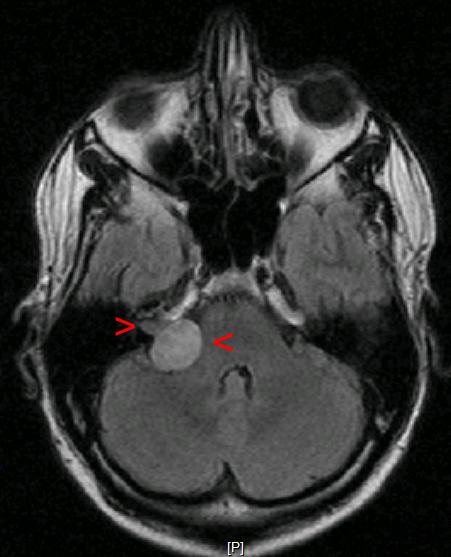
Patient will present as → a 42-year-old male with a history of neurofibromatosis type II, complaining of nausea, vomiting, headache, continuous disequilibrium, and a slowly progressive unilateral hearing loss in his right ear. On physical exam, the patient has decreased sensation to touch on the right side of his face. An MRI is performed, with results seen here.
{kind=link}
An acoustic neuroma (a.k.a. vestibular schwannoma) is a benign tumor of the Schwann cells (the cells that produce myelin sheath), most commonly affecting the vestibular division of the 8th cranial nerve
{kind=link}
- Patients will present with insidious unilateral hearing loss, tinnitus, headache, facial numbness, and continuous disequilibrium
- May cause facial numbness or weakness due to compression of cranial nerve VII (facial nerve)
- Increased incidence in patients with neurofibromatosis type II
- Unilateral hearing loss +/- vertigo
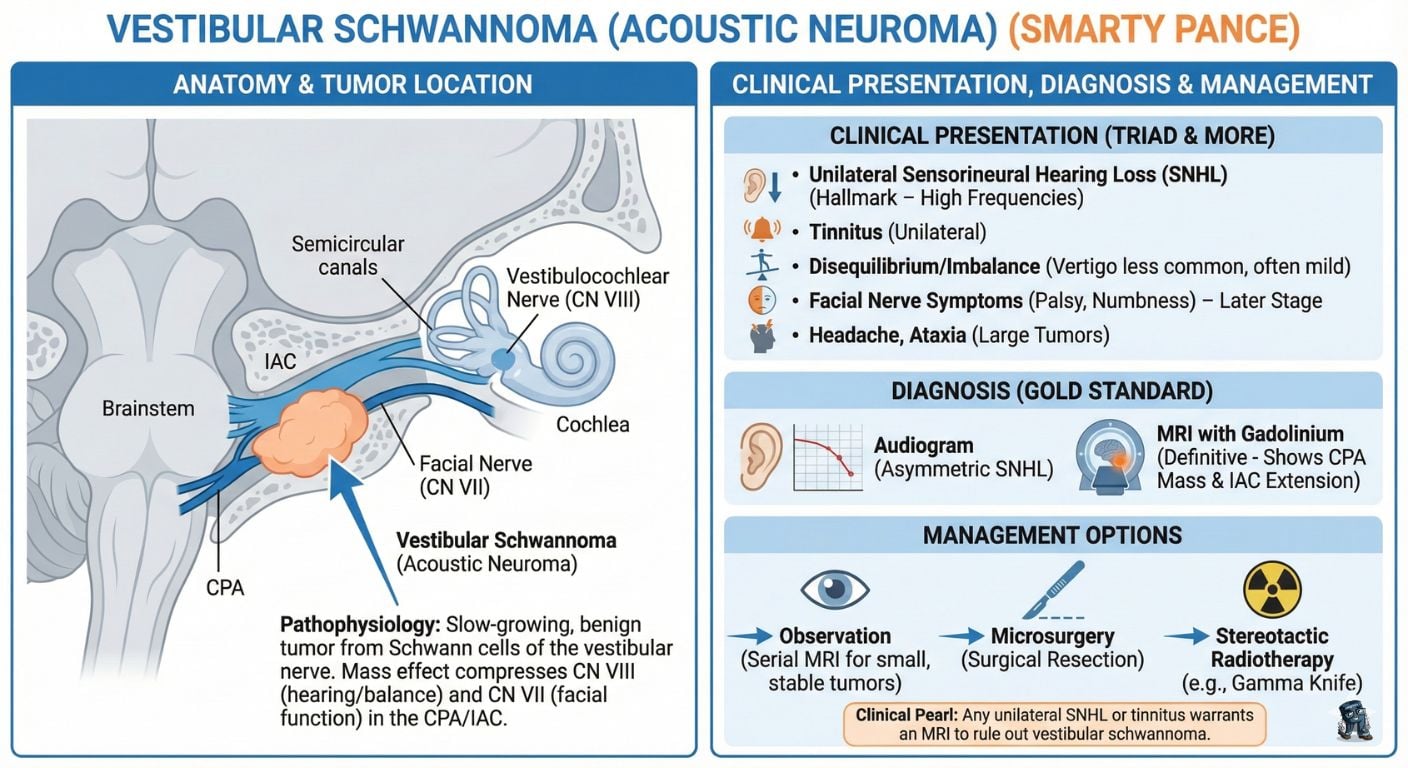
Definitive diagnosis is by MRI (Gold standard)
- An audiogram is the first test done during a physical examination to diagnose acoustic neuroma. It usually reveals an asymmetric sensorineural hearing loss and a greater impairment of speech discrimination than would be expected for the degree of hearing loss
- Such findings indicate the need for imaging tests, preferably gadolinium-enhanced MRI

Acoustic neuroma on right (left image side)
Small or non-growing tumors can be observed with serial MRI scans
- Stereotactic radiation therapy tends to be used for patients who are elderly, those with smaller tumors, or those who cannot undergo surgery for medical reasons.
- Microsurgery can involve a hearing-preservation approach (middle cranial fossa or retrosigmoid approach) or a translabyrinthine approach if there is no useful residual hearing.
Question 1 |
Rinne test: Air conduction (AC) greater than bone conduction (BC) in both ears; Weber test: Lateralizes to the left Hint: Rinne showing AC > BC in both ears with Weber lateralizing to the left would suggest conductive hearing loss in the left ear, which is inconsistent with acoustic neuroma. | |
Rinne test: AC greater than BC in both ears; Weber test: Lateralizes to the right | |
Rinne test: BC greater than AC in the left ear, AC greater than BC in the right ear; Weber test: Lateralizes to the right Hint: Rinne showing BC > AC in the left ear suggests conductive hearing loss, not typical of acoustic neuroma, which is a sensorineural pathology. | |
Rinne test: BC greater than AC in the left ear, AC greater than BC in the right ear; Weber test: Lateralizes to the left Hint: Similar to option C, BC > AC in the left ear indicates conductive hearing loss, not sensorineural. | |
Rinne test: AC equal to BC in both ears; Weber test: No lateralization Hint: AC equal to BC in both ears with no lateralization in the Weber test does not typically indicate unilateral sensorineural hearing loss, as seen in acoustic neuroma. |
Question 2 |
CT scan of the temporal bone Hint: Useful for bone details but less sensitive than MRI for soft tissue lesions like acoustic neuroma. | |
Plain radiography of the skull Hint: Insufficient for diagnosing acoustic neuroma. | |
Ultrasound of the neck Hint: Not useful for diagnosing intracranial lesions. | |
MRI of the brain with gadolinium | |
PET scan Hint: Not typically used in the initial evaluation of acoustic neuroma. |
Question 3 |
Immediate surgical resection Hint: Considered for larger tumors or those causing significant symptoms. | |
Stereotactic radiosurgery Hint: An option for smaller tumors, particularly if they begin to grow or cause more symptoms. | |
Observation with serial imaging | |
Systemic chemotherapy Hint: Not effective for acoustic neuroma. | |
Intratympanic corticosteroid injection Hint: Used for certain inner ear conditions, not for acoustic neuroma. |
|
List |
References: Merck Manual · UpToDate