Patient will present as → a 17-year-old male who returned from a senior class trip to Mexico. While there, they decided to take scuba classes. After 3 days of shallow diving, they attempted their first 100-foot dive. After 5 minutes on their second dive, his equipment failed. He quickly shared the working breathing equipment of his friend, and they rose rapidly to the surface in a panic for air. The patient noticed immediate pain in his right ear, which resolved somewhat when he forcefully yawned and heard a "pop." Since then, he has reported dizziness and hearing loss in the affected ear.
{kind=link}
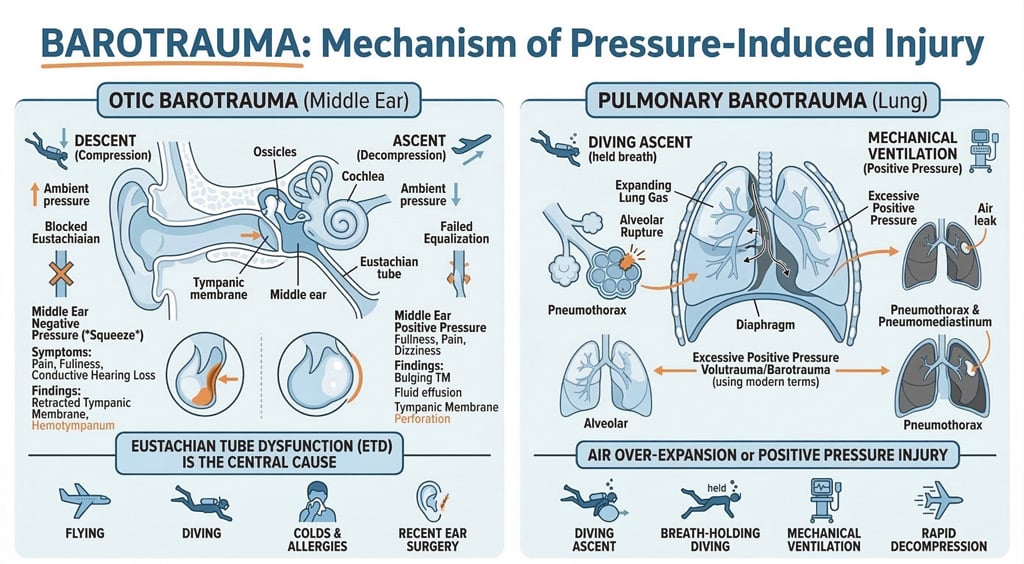
Barotrauma is tissue injury caused by a pressure-related change in body compartment gas volume; it affects air-containing areas, including lungs, ears, sinuses, GI tract, air spaces in tooth fillings, and space contained by the diving face mask
- Symptoms may include ear pain, vertigo, hearing loss, sinus pain, epistaxis, and abdominal pain
- Dyspnea and loss of consciousness are life-threatening and may result from alveolar rupture and pneumothorax

"It’s important to remember that barotrauma and tympanic membrane perforation are not the same thing. Barotrauma is the actual injury caused by a sudden change in pressure across the eardrum—like when diving, flying, or hitting the water hard—and it can cause pain, fullness, or even bleeding behind the eardrum. A tympanic membrane perforation is the physical hole in the eardrum itself, which may result from barotrauma but can also be caused by infections like acute otitis media or direct trauma. In other words, barotrauma is the mechanism, and TM perforation is one of the possible outcomes."
Diagnosis is clinical but sometimes requires imaging tests
- On exam, will see signs of trauma without signs of infection – redness without swelling, pus, or effusion
Treatment is supportive (anti-inflammatories), then consider prophylaxis
- Most barotrauma injuries heal spontaneously
- Urgent surgery (eg, tympanostomy for direct repair of a ruptured round or oval window, myringotomy to drain fluid from the middle ear, sinus decompression) may be necessary for serious inner or middle ear or sinus injuries
- Pseudoephedrine or Afrin can be good for prophylaxis for ear barotrauma – you must be careful when recommending this to divers, depending on dive times
- Risk for overuse – Afrin should not be used for more than 3 days – risk of tachyphylaxis and rhinitis medicamentosa
- Swallowing to open the eustachian tube, along with chewing gum or sucking on hard candies, helps for adults; sucking on a bottle helps for infants
Question 1 |
Continued observation Hint: While many tympanic membrane perforations heal spontaneously, the duration of 12 weeks without healing suggests the need for specialist assessment. | |
An audiogram to document hearing Hint: While documenting hearing is important, the primary concern at this stage is the non-healing perforation, which requires specialist evaluation. | |
Prescribe steroid otic drops Hint: Steroids are not typically used in the management of tympanic membrane perforations and could potentially delay healing or increase the risk of infection. | |
Prescribe antibiotic ear drops and advise against water exposure Hint: Antibiotic drops are generally used in the presence of infection, which is not indicated in this case. While avoiding water exposure is generally advised, the main concern here is the non-healing perforation. | |
Referral to an otolaryngologist (ENT specialist) |
Question 2 |
Transudate of fluid in the middle ear Hint: With negative middle ear pressure, a transudate of fluid may form in the middle ear. | |
Perilymph fistula | |
Rupture of the tympanic membrane (TM) Hint: A very large pressure differential may cause bleeding into the middle ear and TM rupture, as well as the development of a perilymph fistula through the oval or round window. | |
Hemotympanum (bleeding into the middle ear) Hint: A very large pressure differential may cause bleeding into the middle ear and TM rupture, as well as the development of a perilymph fistula through the oval or round window. | |
Eustachian tube dysfunction Hint: While this can cause discomfort and hearing changes due to pressure differences, it typically does not lead to sensorineural hearing loss and vertigo. |
|
List |
References: Merck Manual · UpToDate