

9 m/o with fussiness and decreased oral intake
Patient will present as → a 9-month-old female with nasal congestion and cough is brought to your clinic by her mother who reports that the child is very fussy, has been tugging at her right ear, and refuses to eat. On physical exam, you note copious green/yellow nasal discharge and right-sided otorrhea. An otoscopic exam reveals a significant amount of clear/white discharge obstructing your view. With careful examination, you are able to observe a ruptured right tympanic membrane.
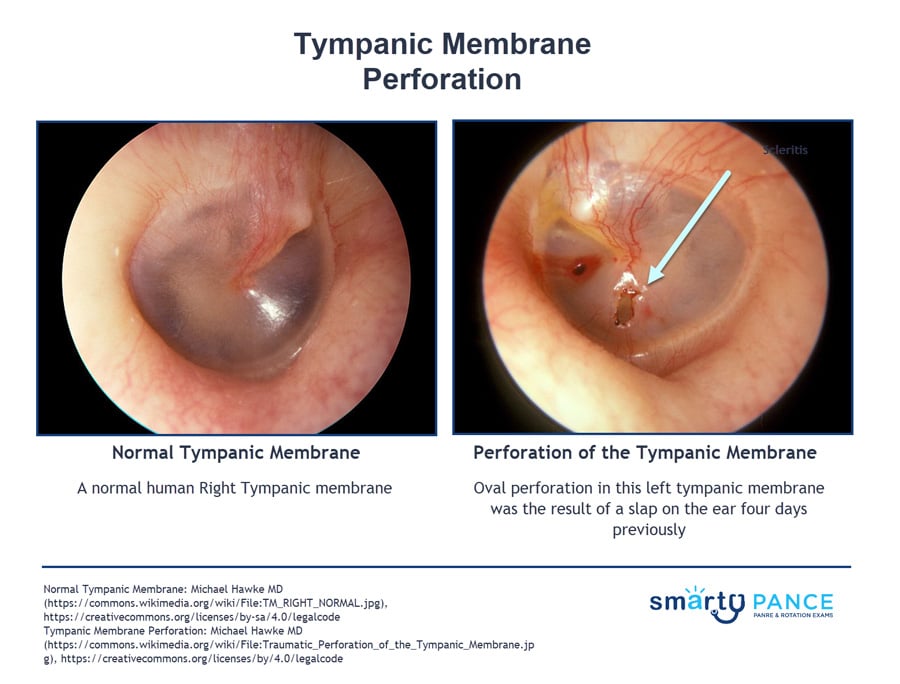
Traumatic perforation of the TM causes sudden severe pain sometimes followed by bleeding from the ear, hearing loss, and tinnitus.
- Most common causes are infection, direct trauma, or barotrauma
- The only class of antibiotics that are non-ototoxic are Floxin drops and should be used if you are going to be prescribing drops with a perforated TM.
- Most TM perforations are nonurgent and do not require immediate evaluation by an otolaryngologist. Often, these can be managed as an outpatient with drops and pain control to decrease inflammation; ENT follow-up in a few days to a week.
- A significant portion of TM perforations heal spontaneously without intervention because of the TM’s regenerative abilities.
- Most are uncomplicated with minimal hearing loss (<40 dB) and lack vestibular complaints.
- Observation of >3 months is a feasible option in select patients with uncomplicated, small perforations.
- Debate exists over dry-ear precautions. But conservatively, patients should avoid getting water into the external auditory canal and into the middle ear space. Typical showering is less of an issue, but swimming in rivers/swimming pools should be avoided until the perforation has healed.
- For patients who participate in water sports as a part of daily life, such as swimmers and divers, repair is recommended to provide the patient a “safe ear.”
- Because there is a connection from the outer ear to the middle ear, dry ear precautions are needed to prevent a nidus of infection such as using a cotton ball in the ear during showers and gentle hairdryer use over-ear if water enters the ear canal.
Diagnosis is based on otoscopy
Patients with small isolated tympanic membrane perforation <25 percent in size and minimal hearing loss (<40 dB, decreased perception of whisper or minor asymmetry):
- Water precautions, topical antibiotic otic drops x 5-7 days, audiometry within 24 hours if not previously obtained, and follow-up with their primary care provider in four weeks to ensure that the perforation is closed and the hearing deficit has been resolved
- The only class of antibiotics that are non-ototoxic are Floxin drops and should be used if you are going to be prescribing drops with a perforated TM
- Surgery may be needed for perforations persisting > 2 mo, disruption of the ossicular chain, or injuries affecting the inner ear
Patients with significant middle ear trauma and hearing loss ≥40 dB, vestibular signs (eg, nystagmus, vomiting, ataxia), findings that indicate basilar skull fracture, or facial nerve injury should undergo emergency evaluation by an otolaryngologist within 48 hours of injury
Question 1 |
Tobramycin otic drops Hint: While effective against Pseudomonas, tobramycin can be ototoxic and is generally avoided if there is a possibility of tympanic membrane perforation. | |
Erythromycin solution Hint: Erythromycin is not typically the first choice for otitis externa, as it has a narrower spectrum of activity against the common pathogens. | |
Offloxacin otic drops | |
Gentamicin drops Hint: Gentamicin is also effective against Pseudomonas but carries a risk of ototoxicity and is not preferred if tympanic membrane status is uncertain. | |
Acetic acid otic solution Hint: Acetic acid solution can be used for mild cases of otitis externa but may not be sufficient for more severe infections, especially when there is significant swelling and discharge. |
Question 2 |
Acute otitis media | |
Foreign body insertion Hint: While foreign bodies can cause TM perforation, especially in children, they are less common than perforations due to AOM. | |
Barotrauma Hint: Barotrauma, such as from diving or flying, can lead to TM perforation, but it is less common compared to AOM. | |
Chronic otitis media Hint: Chronic otitis media can lead to TM perforation, but acute otitis media is a more frequent cause. | |
Loud noise exposure Hint: Exposure to loud noises, such as explosions or gunfire, can cause TM perforation, but these instances are less common compared to AOM. |
Question 3 |
Immediate referral for audiometry Hint: Useful for assessing the extent of hearing loss but not urgent. | |
Prescription of oral antibiotics Hint: Not routinely indicated unless there is evidence of infection. | |
Keep the ear dry and reevaluate in a few weeks | |
CT scan of the temporal bone Hint: Indicated if there is suspicion of more extensive injury. | |
Myringotomy Hint: A surgical procedure not typically required for traumatic tympanic membrane perforation. |
Question 4 |
Continued observation Hint: Not appropriate given the duration and persistent symptoms. | |
Tympanoplasty | |
Systemic corticosteroids Hint: Not effective for tympanic membrane perforation. | |
Topical antibiotic drops Hint: Used to prevent infection but do not facilitate healing of the perforation. | |
Hearing aid fitting Hint: May be considered for permanent hearing loss but after addressing the perforation. |
|
List |
References: Merck Manual · UpToDate