 Lecture
Lecture

14 y/o with blurry vision, unequal pupils, and injected conjunctiva/sclera
Patient will present as → a 14-year-old who sustained a blunt trauma to his right eye after being struck by a baseball. He complains of blurry vision. On physical exam, you note unequal pupils, injected conjunctiva/sclera, and blood in the anterior chamber of the right eye.

To watch this and all of Joe Gilboy PA-C's video lessons you must be a member. Members can log in here or join now.
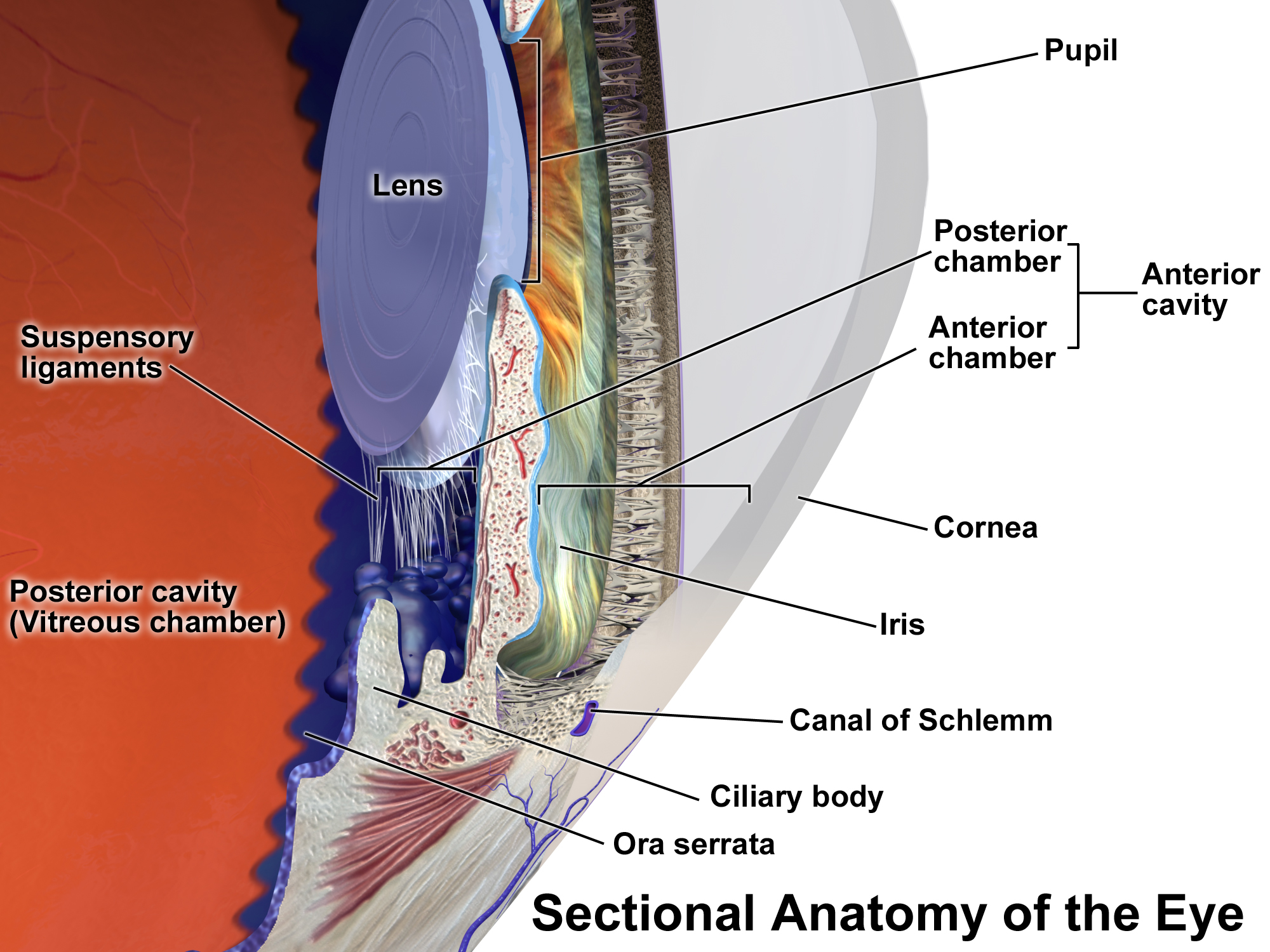
Trauma causes blood in the anterior chamber of the eye (between the cornea and the iris). The blood may cover part or all of the iris (the colored part of the eye) and the pupil, and may partly or totally block vision in that eye.
{kind=link}
- The mechanism of injury varies by age ⇒ usually from blunt/penetrating trauma
- Young children: baseball, softball, soccer, hockey, racquetball, etc.
- Teenagers and adults: assault, paintballs, airbags, bungee cords, etc.
- In trauma ⇒ bleeding results from tears in the vessels of the ciliary body or iris
- In penetrating injury ⇒ bleeding results from direct damage to the iris
- If there is trauma, you need to make sure there is no other type of injury – skull fracture, orbital fracture, etc., etc.

Traumatic hyphema with blood filling approximately half of the anterior chamber. Photo by Rakesh Ahuja, MD via Wikimedia Commons, CC BY-SA 2.5.
Traumatic hyphema is a clinical diagnosis that is made based upon a history of eye trauma and characteristic findings during an ophthalmologic examination
- Orbital CT in patients with a suspected open globe or concern for serious orbital injury
- All patients with a traumatic hyphema warrant prompt evaluation by an ophthalmologist to provide expertise in comprehensive eye examination, including intraocular pressure measurement.
All patients with a traumatic hyphema warrant prompt evaluation by an ophthalmologist to provide expertise in a comprehensive eye examination, including intraocular pressure measurement.
- Frequently, blood is reabsorbed over a period of days to weeks
- Eyeshield - To avoid further injury to the affected eye, an eye shield should be worn at all times until the hyphema resolves or for at least one week
- Elevate the head of the bed at 30 degrees all the time
- Patients with traumatic hyphema receive topical glucocorticoid eye drops
- Daily monitoring of intraocular pressure is a cornerstone in the management of traumatic hyphema
- A normal intraocular pressure (IOP) generally falls within the range of 10-21 mmHg (millimeters of mercury)
- NSAIDs are contraindicated as they may lead to increased bleeding into the anterior chamber
- Surgery if high pressure or persistent bleeding
Question 1 |
Retinal detachment Hint: While retinal detachment can occur due to trauma, it is not a direct complication of hyphema itself. | |
Secondary glaucoma | |
Cataract formation Hint: Cataracts typically develop due to lens changes, which are not directly associated with hyphema. | |
Chronic conjunctivitis Hint: Conjunctivitis is an inflammation of the conjunctiva and is not a typical complication of hyphema. | |
Corneal scarring Hint: While corneal injury can occur with ocular trauma, corneal scarring is not a direct complication of hyphema. |
Question 2 |
Measurement of intraocular pressure | |
Fundoscopic examination Hint: Important for assessing the retina but secondary to intraocular pressure measurement in acute hyphema. | |
CT scan of the orbit Hint: Useful in assessing for orbital fractures but not the immediate concern in isolated hyphema. | |
Fluorescein staining of the cornea Hint: Used to detect corneal abrasions, not directly relevant in hyphema. | |
Visual acuity test Hint: Important but secondary to intraocular pressure measurement in this context. |
Question 3 |
Immediate surgical evacuation of the hyphema Hint: Indicated in cases with high intraocular pressure or sickle cell disease. | |
Patching both eyes Hint: Not recommended as it can increase the risk of amblyopia in children. | |
Topical corticosteroids Hint: May be used to reduce inflammation but are not the primary treatment. | |
Antifibrinolytic therapy Hint: Used in cases with a high risk of re-bleeding. | |
Bed rest with head elevation |
|
List |
References: Merck Manual · UpToDate