
Patient will present as → a 3-year-old who is brought into the emergency room by her parents. The child has had a high fever, sore throat, and stridor. She has a muffled voice and is sitting up on the stretcher drooling while leaning forward with her neck extended. The patient's parents are adamantly against vaccinations, claiming that they are a "government conspiracy." You order a lateral neck x-ray, which shows a swollen epiglottis. The patient recovered following treatment with prednisone and ceftriaxone.
Infection of the upper airway with (most common cause) H. influenzae type B (Hib)
- Presents with classic triad of drooling + dysphagia and distress
- Patients sit with the neck hyperextended and chin protruding (sniffing dog position)
Diagnosis of epiglottitis depends on airway stability, but the approach differs by age:
- Children: If there are signs of distress (stridor, drooling, tripod position, cyanosis), do not attempt to visualize the throat or obtain imaging. Sudden airway collapse can occur with agitation or supine positioning.
- The diagnosis is made clinically and confirmed after airway stabilization during intubation in the OR by an experienced airway team (ENT/anesthesiology)
- Stable older children and adults: May undergo flexible fiberoptic laryngoscopy in a controlled setting (ED, ICU, or OR), showing a swollen, cherry-red epiglottis
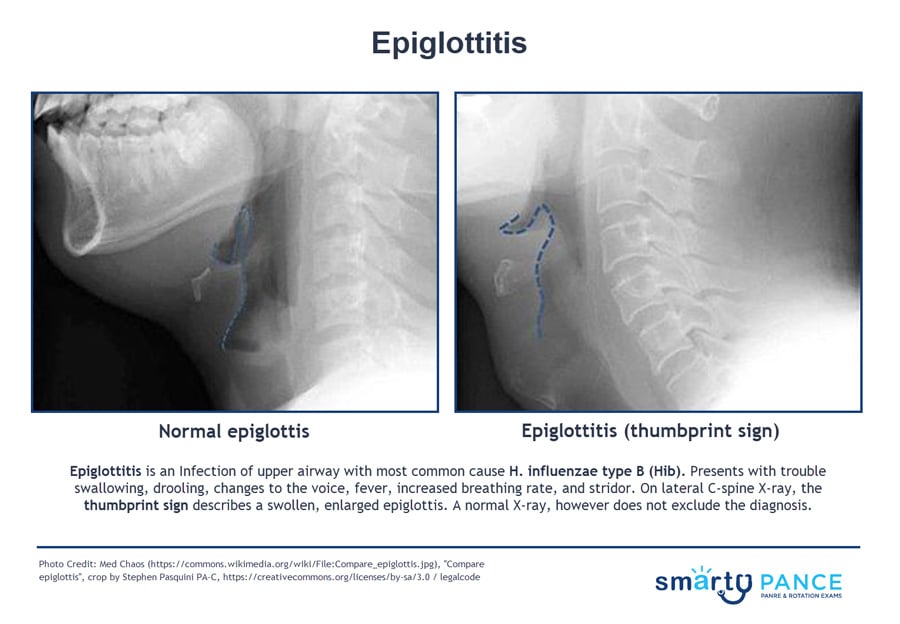
- A lateral neck X-ray can demonstrate the thumbprint sign but is not required if clinical suspicion is high
Key point: In children, never delay airway management for imaging or throat examination—keep the patient calm, seated upright, and involve airway experts early
Secure airway - call anesthesiology and prepare to establish airway, transfer to OR to perform an exam, tracheostomy if necessary to maintain airway
- Admit for observation, humidified O2, IV antibiotics (ceftriaxone + clindamycin), and IV corticosteroids
 Osmosis Osmosis |
|
 |
 Epiglottitis is supraglottic inflammation/obstruction of the airway due to infection with Haemophilus influenzae. The Hib vaccine is available to protect against Haemophilus influenzae type b and should be given to infants in three to four divided doses starting at the age of two months. Signs and symptoms of epiglottitis include inspiratory stridor, restlessness, cough, dyspnea, fever, and drooling. It is important to note that the throat should not be examined if epiglottitis is suspected, as this could cause spasm and complete closure of the airway. Assessment of the throat should only be done when immediate endotracheal intubation is possible. Epiglottitis requires emergency treatment.
Epiglottitis is supraglottic inflammation/obstruction of the airway due to infection with Haemophilus influenzae. The Hib vaccine is available to protect against Haemophilus influenzae type b and should be given to infants in three to four divided doses starting at the age of two months. Signs and symptoms of epiglottitis include inspiratory stridor, restlessness, cough, dyspnea, fever, and drooling. It is important to note that the throat should not be examined if epiglottitis is suspected, as this could cause spasm and complete closure of the airway. Assessment of the throat should only be done when immediate endotracheal intubation is possible. Epiglottitis requires emergency treatment.
| Epiglottitis assessment | Play Video + Quiz |
| Epiglottitis interventions | Play Video + Quiz |
| Haemophilus influenzae disease | Play Video + Quiz |
| Third-generation cephalosporin | Play Video + Quiz |
Question 1 |
Croupy cough and drooling | |
Thick gray, adherent exudate Hint: Thick gray adherent exudate is suggestive of diphtheria. | |
Beefy red uvula, palatal petechiae, white exudate Hint: Beefy red uvula, palatal petechiae, and white exudate are findings suggestive of streptococcal pharyngitis. | |
Inflammation and medial protrusion of one tonsil Hint: Inflammation with medial protrusion of the tonsil is suggestive of a peritonsillar abscess. |
Question 2 |
Rhinovirus Hint: Causes upper respiratory infections but not a common cause of epiglottitis. | |
Streptococcus pneumoniae Hint: Can infect the respiratory tract but not a prime cause of epiglottitis. | |
Neisseria meningitidis Hint: Associated with meningitis more than epiglottitis. | |
Haemophilus influenzae type B | |
Group A Streptococcus Hint: Leads to pharyngitis and tonsillitis more often than epiglottitis. |
Question 3 |
Throat culture Hint: Difficult to obtain and does not provide specific information in this case. | |
Lateral neck X-ray | |
Complete blood count Hint: Not specific for diagnosing epiglottitis. | |
Monospot test Hint: Checks for EBV infection unrelated to this child's presentation. | |
Rapid streptococcal test Hint: Useful for pharyngitis but not epiglottitis. |
Question 4 |
Intravenous antibiotics Hint: Treat the underlying infection but do not address the airway obstruction. | |
Nebulized racemic epinephrine Hint: May transiently improve stridor but intubation is still required. | |
Intubation | |
Oral corticosteroids Hint: Do not improve the airway obstruction requiring intubation | |
Cool mist humidification Hint: May provide some symptomatic relief but does not address need for intubation. |
|
List |
References: Merck Manual · UpToDate