 Lecture
Lecture

47-year-old with pharyngitis and difficulty swallowing
Patient will present as → a 19-year-old male who you are seeing for follow-up from the urgent care, where he was seen 2 days earlier with a sore throat. The patient is febrile (102°F), has a muffled (hot potato) voice, and has extreme difficulty opening his mouth (trismus). He opens it just far enough for you to note uvular deviation.
{kind=link}

To watch this and all of Joe Gilboy PA-C's video lessons, you must be a member. Members can log in here or join now.
A peritonsillar abscess is a complication of tonsillitis and occurs when a collection of pus forms and spreads beyond the tonsils into the tissues of the throat next to one of the tonsils. Swollen tissues can block the airway
- A peritonsillar abscess can present with a significant sore throat, pain with swallowing, trismus (inability to open the mouth normally), deviation of the soft palate/uvula, and a muffled “hot potato” voice
- Deviation of the soft palate and an asymmetric rise of the uvula is highly suggestive of abscess
- Also known as “Quincy's” abscess
- It usually involves multiple bacteria. Streptococcus and Staphylococcus are the most frequent aerobic pathogens, whereas Bacteroides sp is the predominant anaerobic pathogen
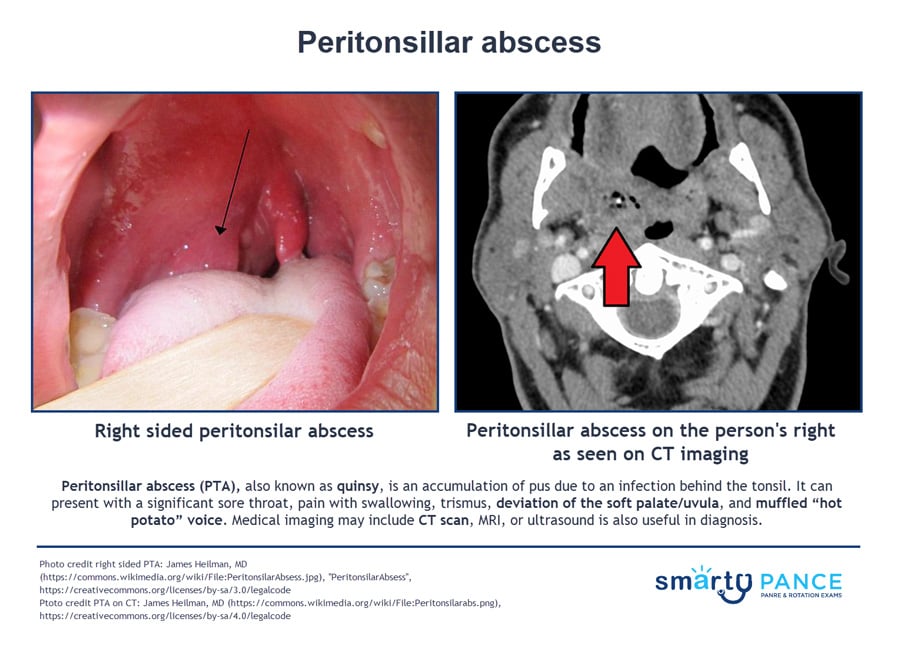
CT or ultrasonography of the neck (which would show the collection of pus within the tissue) can help confirm the diagnosis when the physical examination is difficult, or the diagnosis is in doubt, particularly when the condition must be differentiated from a parapharyngeal infection or other deep neck infection
- Ultrasound (preferred imaging) – Intraoral or transcutaneous ultrasound can confirm the presence of a fluid collection and guide drainage. It also helps differentiate peritonsillar cellulitis (no pus collection) from an abscess (pus present)
- CT with contrast (when to order):
- Diagnosis is uncertain
- Concern for deep neck infection (e.g., parapharyngeal or retropharyngeal abscess)
- Patient exam is limited (e.g., severe trismus, young child)
- Needle aspiration – If performed, aspiration of pus confirms abscess, whereas absence of pus suggests cellulitis. Aspirated fluid should be sent for culture and sensitivity
- Small (< 1 cm): antibiotics alone ± single IV dose, close follow-up in 24–36 hr
- Moderate–large (≥ 1 cm, trismus, toxic features): IV antibiotics + drainage
- Airway compromise: secure the airway before attempting drainage or giving antibiotics
- Tonsillectomy: for recurrent abscess, obstruction, or failed drainage
- Mnemonic: “PTA = Protect airway, Treat with antibiotics, Aspirate”
Management of peritonsillar abscess (PTA) depends on severity, abscess size, and airway status
- Airway comes first – Patients with stridor, drooling, severe trismus, or respiratory distress need immediate airway protection (ENT/airway specialist → OR for intubation and drainage)
- Drainage is definitive – Most PTAs require needle aspiration (preferred) or incision & drainage (I&D) combined with antibiotics. Tonsillectomy is reserved for recurrent PTA, airway obstruction, or failed drainage
- Antibiotic therapy (14 days total) – Empiric therapy should cover Group A strep, Staphylococcus, and anaerobes:
- IV options (moderate/large abscess, systemic illness): ampicillin-sulbactam or clindamycin. Add vancomycin if MRSA risk
- Oral options (small abscess, cellulitis, outpatient bridge after drainage): amoxicillin-clavulanate or clindamycin
- When antibiotics alone may be reasonable:
- Peritonsillar cellulitis (no abscess on US/exam)
- Small abscess < 1 cm with minimal trismus and mild symptoms
- Must have reliable follow-up in 24–36 hours
- Supportive care – Analgesia, hydration, and monitoring for complications (airway compromise, aspiration pneumonia, sepsis, Lemierre syndrome)
- Steroids may reduce pain and edema, but evidence is mixed. Some NT specialists use a single IV dose (e.g., dexamethasone), but this is not universally recommended
 Osmosis Osmosis |
|
 |
Question 1 |
Recurrent streptococcal pharyngitis Hint: This presentation suggests a complication of an incompletely treated streptococcal pharyngitis rather than recurrent disease. | |
Infectious mononucleosis Hint: Infectious mononucleosis may present with severe sore throat, fever, and cervical adenopathy in this age group, but would not cause deviation of the soft palate or the muffled voice. | |
Gonococcal pharyngitis Hint: Gonococcal pharyngitis usually follows a more indolent course than this patient's presentation. | |
Peritonsillar abscess |
Question 2 |
CBC with differential Hint: A CBC with differential would identify an infection but not specifically a retropharyngeal abscess. | |
fever and a muffled voice on examination Hint: The presence of fever and a muffled voice on physical exam is not specific for a retropharyngeal abscess. | |
CT of the neck with contrast | |
history of a recent throat infection Hint: A recent throat infection is not specific for a retropharyngeal abscess. |
Question 3 |
Needle aspiration | |
Corticosteroid administration Hint: Corticosteroids, nebulized epinephrine, and nasotracheal intubation are not indicated in the treatment of peritonsillar abscesses. | |
Nebulized epinephrine administration Hint: Corticosteroids, nebulized epinephrine, and nasotracheal intubation are not indicated in the treatment of peritonsillar abscesses. | |
Nasotracheal intubation Hint: Corticosteroids, nebulized epinephrine, and nasotracheal intubation are not indicated in the treatment of peritonsillar abscesses. |
|
List |
References: Merck Manual · UpToDate